Proximal Humerus Fracture ORIF (Plate and Nail Fixation) PDF Evidence¶
Why this operation has been suggested¶
Open reduction and internal fixation is a surgery to realign broken bones and hold them in place with plates and screws. Your surgeon may have suggested this for you because non-operative options, such as rest and immobilization, have not provided enough improvement. While many patients heal well without surgery, your specific fracture pattern likely requires mechanical stability to ensure proper healing. This approach is particularly considered for displaced fractures where the bone fragments have shifted out of their natural position.
The main goal of this operation is to restore stability to your shoulder, which helps reduce pain and improves your ability to use your arm. For patients with healthy bone density, this method can provide favorable long-term results. However, it is important to understand the risks. In patients over 60, there is a 44% complication rate and a 34% failure rate. You must remain in a sling and must not drive for at least six weeks after surgery. Once your surgeon clears you, typically at the six-week review, you may resume driving. For more details, see Driving after upper-limb surgery.
Before the operation¶
Please fast for eight hours before your surgery. Stop taking blood thinners only after your surgeon advises. Arrange a ride home, as you cannot drive for at least six weeks after any shoulder operation. Bring a list of all current medications and wear comfortable, loose clothing. You may need X-rays, blood tests, or an anaesthetic review to check your health and plan the surgery. Your surgeon will use an open approach with a single incision over the shoulder. This allows direct access to fix the fracture with a plate and screws. Follow your surgeon’s specific instructions for medication changes and arrival time.
On the day¶
This operation is done under general anaesthetic combined with a regional nerve block. You will be fully asleep for the operation, and the block — an injection that numbs the nerves supplying the arm before you wake up — provides pain relief for the first 12 to 24 hours after surgery. The anaesthetist will meet you before the operation and talk you through both parts.
You will arrive at the hospital and be admitted to a ward. Your surgeon will make a single conventional incision over the operative site to fix the fracture. You will then go to the operating theatre. After the procedure, you will wake up in recovery. Your arm will be in a sling. You must not drive for at least six weeks after any shoulder operation, regardless of which arm was operated on. Once your surgeon clears you, typically at the six-week review, you may resume driving. For more details, see Driving after upper-limb surgery.
What the operation involves¶
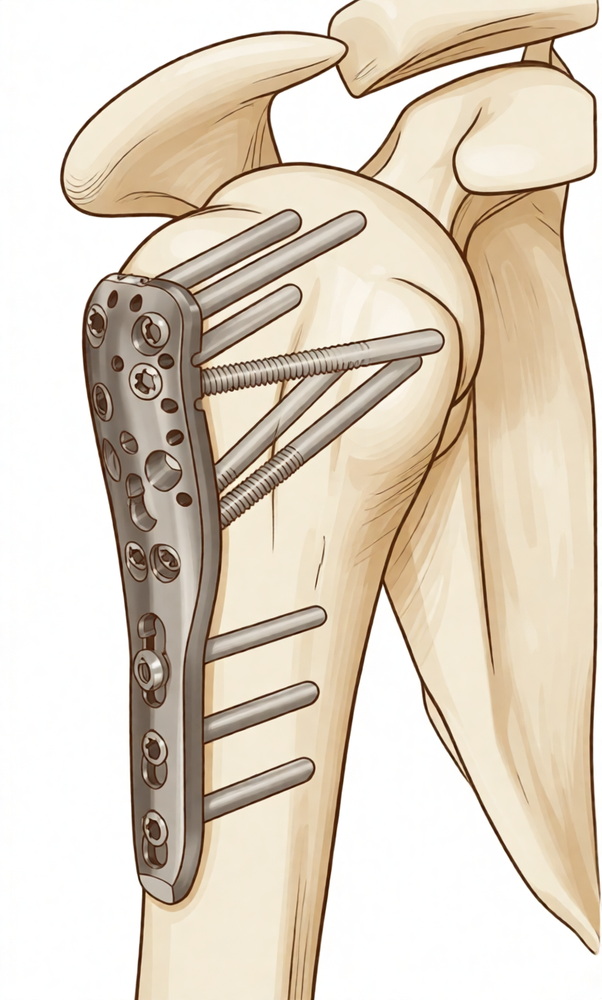
Your surgeon makes a single cut about 8 to 10 cm long over the front of your shoulder. This open approach gives clear access to the broken bone. Through this incision, your surgeon carefully moves tissues aside to see the fracture site.
The broken pieces of your upper arm bone are realigned into their correct position. Your surgeon then uses a metal plate and screws to hold the bone fragments together. This plate acts like an internal splint, keeping the bone stable while it heals. In some cases, a metal rod may be placed inside the center of the bone shaft to provide support. This rod is secured with screws at the top and bottom.
Your surgeon checks that the fixation is strong and secure. The cut is then closed with stitches or staples. A sterile dressing is applied to protect the wound.
The operation typically takes between one and two hours. You will have a sling to support your arm after the procedure. You must not drive for at least six weeks after this surgery, regardless of which arm was operated on. You should wait until your surgeon clears you, typically at the six-week review, before driving again. For more details, see Driving after upper-limb surgery.
After the operation¶
You will wake up in the recovery ward with your arm in a sling and a dressing over the incision. Your surgeon will manage your pain to keep you comfortable. You should have someone stay with you for the first 24 hours. Most patients go home the same day or after an overnight stay. You must not drive for at least six weeks after any shoulder operation, regardless of which arm was operated on. You can drive once your surgeon clears you, typically at the six-week review. See Driving after upper-limb surgery for more details. Keep the dressing clean and dry until your next appointment.
Recovery¶
You will have a single incision over your shoulder. In the first few days, pain and swelling are normal. Your surgeon will prescribe medication to keep you comfortable. Resting with your arm supported helps reduce swelling. You will wear a sling to protect the repair. Keep it on as directed.
Your physiotherapist will guide your exercises. Early movement is important for healing. You will start gentle motions soon after surgery. This helps prevent stiffness. Do not lift heavy objects or reach overhead until your surgeon clears you. Simple tasks like eating or brushing your teeth may be possible with your non-operated arm.
Sleeping may be difficult at first. Try propping yourself up with pillows. This takes pressure off the shoulder. As pain settles and movement returns, you will gradually increase activity. You can return to driving once your surgeon clears you, typically at the six-week review. See Driving after upper-limb surgery for more details.
Your timeline may differ. Your surgeon and physio will guide you based on your healing progress. Most patients return to baseline function by one year. Consistent effort with your exercises supports the best outcome.
What can go wrong¶
Most patients do well, but problems can occasionally happen. Your surgeon and the team monitor you closely to spot any issue early.
Infection is a serious risk after this surgery. You might notice a deep, throbbing pain that does not ease with simple painkillers. The skin around your incision may become red, warm, or swollen. You might see pus or unusual drainage from the wound. If you have a fever or chills, contact your clinic immediately. This is a devastating complication that can affect your recovery.
Your bone may not heal properly. This is called nonunion. You might feel persistent pain at the fracture site when you try to move your arm. The bone fragments might shift, causing a clicking or grinding feeling. Your surgeon will check for this during your follow-up visits.
The blood supply to the head of your upper arm bone can be damaged. This is known as avascular necrosis. You may experience a deep ache in your shoulder that worsens over time. Your range of motion might decrease. You might notice stiffness that feels different from normal post-surgery soreness. Report any new, deep pain to your surgeon.
The hardware used to hold your bones together can fail. This includes the plate or screws loosening or breaking. You might feel a sudden change in how your shoulder feels. There could be a popping sensation or a loss of stability. If your arm feels weak or unstable, seek medical advice right away.
Reoperation is more likely if your fracture involved a dislocation. This means the ball of the shoulder joint came out of the socket. You might notice instability or a feeling that the joint is slipping. If you experience this, contact your surgeon promptly.
Older patients face higher risks from surgery itself. Inpatient adverse events and mortality are higher for those over 60. You might experience general weakness, confusion, or breathing difficulties while in the hospital. These are serious signs that require immediate attention from your care team.
The complications table on this page lists typical rates if you want the specifics.
When to call us¶
Call us if you have a fever, increasing wound redness, or discharge. Seek emergency care for sudden severe pain, calf swelling, or shortness of breath. Contact us immediately if you lose sensation or cannot move your limb. These signs need urgent assessment to prevent serious complications.
Evidence & references
title: "Proximal Humerus Fracture ORIF (Plate and Nail Fixation)" slug: proximal-humerus-orif region: shoulder audience: patient mesh_terms: ["Shoulder Fractures", "Bone Plates", "Bone Nails"] article_count: 1706 model_used: Qwen3.6-35B-A3B-Q8_0.gguf generated_at: '2026-06-14T15:37:49+00:00' key_articles: - title: "Locking plate fixation of proximal humerus fractures in patients older than 60 years continues to be associated with a high complication rate" ref_num: 1 evidence_tier: paper evidence_level: 4 doi: 10.1016/j.jse.2019.11.026 year: 2020 - title: "What Are the Long-term Outcomes of Locking Plates for Nonosteoporotic Three-part and Four-part Proximal Humeral Fractures With a Minimum 10-year Follow-up Period?" ref_num: 2 evidence_tier: paper evidence_level: 3 doi: 10.1097/corr.0000000000002895 year: 2023 - title: "Similar Outcomes for Nail versus Plate Fixation of Three-part Proximal Humeral Fractures" ref_num: 3 evidence_tier: paper evidence_level: 2 doi: 10.1007/s11999-011-2056-y year: 2012 - title: "Complications and Long-Term Outcomes of Open Reduction and Plate Fixation of Proximal Humeral Fractures" ref_num: 4 evidence_tier: paper evidence_level: 4 doi: 10.2106/jbjs.19.00595 year: 2019 - title: "Outcomes after percutaneous reduction and fixation of proximal humeral fractures" ref_num: 5 evidence_tier: paper evidence_level: 4 doi: 10.1016/j.jse.2006.09.006 year: 2007 - title: "Locking intramedullary nails compared with locking plates for two- and three-part proximal humeral surgical neck fractures: a randomized controlled trial" ref_num: 6 evidence_tier: paper evidence_level: 1 doi: 10.1016/j.jse.2016.02.003 year: 2016 - title: "The results of ORIF of displaced unstable proximal humeral fractures using a locking plate" ref_num: 7 evidence_tier: paper evidence_level: 2 doi: 10.1016/j.jse.2009.08.008 year: 2010 - title: "Reverse total shoulder arthroplasty for failed open reduction and internal fixation of fractures of the proximal humerus" ref_num: 8 evidence_tier: paper evidence_level: 4 doi: 10.1016/j.jse.2016.05.020 year: 2017 - title: "Four-part valgus impacted proximal humeral fracture presenting three months after injury in a young patient: Open reduction and internal fixation with triple osteotomy and bone graft augmentation" ref_num: 9 evidence_tier: paper evidence_level: 4 doi: 10.1016/j.jse.2007.12.012 year: 2009 - title: "Outcomes of AO/OTA C-type fractures of the distal humerus after open reduction and internal fixation with locking plate constructs in patients at least 65 years old" ref_num: 10 evidence_tier: paper evidence_level: 3 doi: 10.1186/s12891-022-05431-5 year: 2022 - title: "Quality of life and functional outcome after a 2-part proximal humeral fracture: A prospective cohort study on 50 patients treated with a locking plate" ref_num: 11 evidence_tier: paper evidence_level: 4 doi: 10.1016/j.jse.2009.11.046 year: 2010 - title: "Treatment choice affects inpatient adverse events and mortality in older aged inpatients with an isolated fracture of the proximal humerus" ref_num: 12 evidence_tier: paper evidence_level: 3 doi: 10.1016/j.jse.2013.09.006 year: 2014 - title: "Effect of intramedullary nail and locking plate in the treatment of proximal humerus fracture: an update systematic review and meta-analysis" ref_num: 13 evidence_tier: paper evidence_level: 1 doi: 10.1186/s13018-019-1345-0 year: 2019 - title: "Fracture dislocations of the proximal humerus treated with open reduction and internal fixation: a systematic review" ref_num: 14 evidence_tier: paper evidence_level: 4 doi: 10.1016/j.jse.2022.04.018 year: 2022 - title: "Double plating with autogenous bone grafting as a salvage procedure for recalcitrant humeral shaft nonunion" ref_num: 15 evidence_tier: paper evidence_level: 4 doi: 10.1186/s12891-020-03743-y year: 2020 - title: "Purchase of both proximal and distal fragments by the calcar screw is critical when using a locking plate in the treatment of proximal humeral fractures" ref_num: 16 evidence_tier: paper evidence_level: 3 doi: 10.1302/0301-620x.107b9.bjj-2024-1649.r1 year: 2025 - title: "Three- and Four-Part Proximal Humerus Fractures: Open Reduction and Internal Fixation Versus Arthroplasty" ref_num: 17 evidence_tier: paper evidence_level: 5 doi: 10.1016/j.jhsa.2010.07.019 year: 2010 - title: "Intramedullary Fixation for Proximal Humeral Fractures" ref_num: 18 evidence_tier: paper evidence_level: 4 doi: 10.5435/jaaos-d-18-00360 year: 2020 - title: "A New Locking Plate for Unstable Fractures of the Proximal Humerus" ref_num: 19 evidence_tier: paper evidence_level: 2 doi: 10.1097/01.blo.0000137554.91189.a9 year: 2005 - title: "Readmissions, revisions, and mortality after treatment for proximal humeral fractures in three large states" ref_num: 20 evidence_tier: paper evidence_level: 3 doi: 10.1186/s12891-019-2812-9 year: 2019 - title: "Elective implant removal in symptomatic patients after internal fixation of proximal humerus fractures improves clinical outcome" ref_num: 21 evidence_tier: paper evidence_level: 4 doi: 10.1186/s12891-016-0977-z year: 2016 - title: "Delays beyond 5 days to surgery does not affect outcome following plate and screw fixation of proximal humerus fractures" ref_num: 22 evidence_tier: paper evidence_level: 3 doi: 10.1016/j.jse.2025.02.019 year: 2025 - title: "Fixed-angle Locked Plating of Two-, Three-, and Four-part Proximal Humerus Fractures" ref_num: 23 evidence_tier: paper evidence_level: 4 doi: 10.5435/00124635-200805000-00008 year: 2008 - title: "Locking plate fixation for proximal humeral fractures: Initial results with a new implant" ref_num: 24 evidence_tier: paper evidence_level: 4 doi: 10.1016/j.jse.2006.06.006 year: 2007 - title: "Outcomes of open reduction and internal fixation of proximal humerus fracture dislocations" ref_num: 27 evidence_tier: paper evidence_level: 4 doi: 10.1016/j.jse.2021.01.025 year: 2021 - title: "Wound complications after distal humerus fracture fixation: incidence, risk factors, and outcome" ref_num: 28 evidence_tier: paper evidence_level: 4 doi: 10.1016/j.jse.2013.09.014 year: 2014 - title: "The role of greater tuberosity healing in reverse shoulder arthroplasty: a finite element analysis" ref_num: 30 evidence_tier: paper evidence_level: 5 doi: 10.1016/j.jse.2019.07.022 year: 2020 - title: "Does objective shoulder impairment explain patient-reported functional outcome? A study of proximal humerus fractures" ref_num: 31 evidence_tier: paper evidence_level: 3 doi: 10.1016/j.jse.2010.06.005 year: 2011 - title: "Neer Award 2006: Biomechanical assessment of inferior tuberosity placement during hemiarthroplasty for four-part proximal humeral fractures" ref_num: 32 evidence_tier: paper evidence_level: 5 doi: 10.1016/j.jse.2007.06.017 year: 2008 - title: "A scoping review of biomechanical testing for proximal humerus fracture implants" ref_num: 33 evidence_tier: paper evidence_level: 4 doi: 10.1186/s12891-015-0627-x year: 2015 - title: "Mechanical study of the safe distance between humerus shaft fracture and distal locking screws in antegrade nailing" ref_num: 34 evidence_tier: paper evidence_level: 5 doi: 10.1186/s12891-025-08711-y year: 2025 - title: "Finite element analysis of the treatment of a minimally invasive approach combined with a novel anatomical locking plate for scapular body fractures" ref_num: 35 evidence_tier: paper evidence_level: 5 doi: 10.1186/s13018-024-04905-7 year: 2024 - title: "Assessment of fracture stability following modified minimally invasive reduction osteosynthesis system (MIROS) fixation for Neer 2 and 3-Part proximal humeral fractures" ref_num: 36 evidence_tier: paper evidence_level: 3 doi: 10.1186/s12891-025-08600-4 year: 2025 - title: "Postoperative treatment of proximal humerus fractures with an early active motion protocol: a prospective randomized controlled trail" ref_num: 38 evidence_tier: paper evidence_level: 2 doi: 10.1016/j.jse.2025.01.042 year: 2025 - title: "Improvement in shoulder rotation in complex shoulder fractures treated by reverse shoulder arthroplasty" ref_num: 39 evidence_tier: paper evidence_level: 3 doi: 10.1016/j.jse.2012.03.011 year: 2013 - title: "Evaluation of the Constant score: which is the method to assess the objective strength?" ref_num: 42 evidence_tier: paper evidence_level: 3 doi: 10.1186/s12891-019-2795-6 year: 2019 - title: "Does fracture of the dominant shoulder have any effect on functional and quality of life outcome compared with the nondominant shoulder?" ref_num: 44 evidence_tier: paper evidence_level: 3 doi: 10.1016/j.jse.2014.10.006 year: 2015 - title: "Management of clavicle nonunion and malunion" ref_num: 45 evidence_tier: paper evidence_level: 5 doi: 10.1016/j.jse.2013.01.022 year: 2013 - title: "A clinical study on robot navigationassisted intramedullary nail treatment for humeral shaft fractures" ref_num: 46 evidence_tier: paper evidence_level: 3 doi: 10.1186/s12891-024-07848-6 year: 2024 - title: "The assessment of scapular radiographs" ref_num: 47 evidence_tier: paper evidence_level: 4 doi: 10.1302/0301-620x.95b8.30631 year: 2013 - title: "Different suture anchor fixation techniques affect contact properties in humeral greater tuberosity fracture: a biomechanical study" ref_num: 48 evidence_tier: paper evidence_level: 5 doi: 10.1186/s12891-019-2412-8 year: 2019 - title: "Altered Glenohumeral Biomechanics in Proximal Humeral Fracture Malunion" ref_num: 49 evidence_tier: paper evidence_level: 5 doi: 10.5435/jaaos-d-20-00555 year: 2020 - title: "STABILIZATION OF PROXIMAL HUMERAL FRACTURES WITH AN ANGULAR AND SLIDING STABLE ANTEGRADE LOCKING NAIL (TARGON PH)" ref_num: 50 evidence_tier: paper evidence_level: 4 doi: 10.2106/00004623-200300004-00019 year: 2003 - title: "Functional outcome following one-part proximal humeral fractures: A prospective study" ref_num: 51 evidence_tier: paper evidence_level: 3 doi: 10.1016/j.jse.2007.07.016 year: 2008 - title: "Early functional improvements using continuous passive motion therapy after angular-stable plate osteosynthesis of proximal humerus fractures – results of a prospective, randomized trial" ref_num: 52 evidence_tier: paper evidence_level: 1 doi: 10.1186/s13018-024-04804-x year: 2024 - title: "Modified minimally invasive approach and intra-osseous portal for three-part proximal humeral fractures: a comparative study" ref_num: 53 evidence_tier: paper evidence_level: 3 doi: 10.1186/s13018-017-0701-1 year: 2018 - title: "Open reduction and internal fixation of humeral midshaft fractures: anterior versus posterior plate fixation" ref_num: 54 evidence_tier: paper evidence_level: 3 doi: 10.1186/s12891-019-2888-2 year: 2019 - title: "A novel surgical approach and technique and short-term clinical efficacy for the treatment of proximal humerus fractures with the combined use of medial anatomical locking plate fixation and minimally invasive lateral locking plate fixation" ref_num: 56 evidence_tier: paper evidence_level: 4 doi: 10.1186/s13018-020-02094-7 year: 2021 - title: "Operative versus non-operative treatment for 2-part proximal humerus fracture: A multicenter randomized controlled trial" ref_num: 59 evidence_tier: paper evidence_level: 1 doi: 10.1371/journal.pmed.1002855 year: 2019 - title: "Contemporary Management of Proximal Humeral Fractures" ref_num: 60 evidence_tier: paper evidence_level: 5 doi: 10.5435/jaaos-d-24-01073 year: 2025 - title: "Kirschner wire versus external fixation in the treatment of proximal humeral fractures in older children and adolescents: a comparative study" ref_num: 62 evidence_tier: paper evidence_level: 3 doi: 10.1186/s12891-023-07037-x year: 2023 - title: "One Versus 3-Week Immobilization Period for Nonoperatively Treated Proximal Humeral Fractures" ref_num: 63 evidence_tier: paper evidence_level: 2 doi: 10.2106/jbjs.20.02137 year: 2021 - title: "CORR Insights®: What Factors Are Associated With Poor Shoulder Function and Serious Complications After Internal Fixation of Three-part and Four-part Proximal Humerus Fracture-dislocations?" ref_num: 64 evidence_tier: paper evidence_level: 5 doi: 10.1097/corr.0000000000002242 year: 2022 - title: "Biomechanical evaluation of locked plating in proximal humeral fractures" ref_num: 66 evidence_tier: paper evidence_level: 5 doi: 10.1016/j.jse.2006.03.013 year: 2007 - title: "Long-term functional outcomes (median 10 years) after locked plating for displaced fractures of the proximal humerus" ref_num: 67 evidence_tier: paper evidence_level: 4 doi: 10.1016/j.jse.2013.11.009 year: 2014 - title: "DUAL SLOTTED PLATES IN FIXATION OF FRACTURES OF THE FEMORAL SHAFT" ref_num: 68 evidence_tier: paper evidence_level: 4 doi: 10.2106/00004623-196345020-00026 year: 1963 - title: "Cost-Minimization Analysis and Treatment Trends of Surgical and Nonsurgical Treatment of Proximal Humerus Fractures" ref_num: 69 evidence_tier: paper evidence_level: 4 doi: 10.1016/j.jhsa.2020.03.022 year: 2020 - title: "Intramedullary nailing of the proximal humerus: evolution, technique, and results" ref_num: 70 evidence_tier: paper evidence_level: 5 doi: 10.1016/j.jse.2015.11.016 year: 2016 - title: "Long Philos Plate Fixation for Complex Humeral Fractures" ref_num: 71 evidence_tier: paper evidence_level: 4 doi: 10.1111/j.1758-5740.2010.00085.x year: 2010 - title: "Locking plate versus nonsurgical treatment for proximal humeral fractures: better midterm outcome with nonsurgical treatment" ref_num: 72 evidence_tier: paper evidence_level: 3 doi: 10.1016/j.jse.2011.01.025 year: 2011 - title: "Proximal Humeral Fracture Treatment in Adults" ref_num: 73 evidence_tier: paper evidence_level: 5 doi: 10.2106/jbjs.l.01293 year: 2014 - title: "The effect of medial calcar support on proximal humeral fractures treated with locking plates" ref_num: 76 evidence_tier: paper evidence_level: 3 doi: 10.1186/s13018-022-03337-5 year: 2022 - title: "Functional and radiographic medium-term outcome evaluation of the Humerus Block, a minimally invasive operative technique for proximal humeral fractures" ref_num: 78 evidence_tier: paper evidence_level: 4 doi: 10.1016/j.jse.2011.07.029 year: 2012 - title: "A comprehensive classification of proximal humeral fractures: HGLS system" ref_num: 79 evidence_tier: paper evidence_level: 3 doi: 10.1016/j.jse.2012.09.018 year: 2013 - title: "Can patient and fracture factors predict opioid dependence following upper extremity fractures?: a retrospective review" ref_num: 80 evidence_tier: paper evidence_level: 3 doi: 10.1186/s13018-019-1233-7 year: 2019 - title: "Locked Plating of Proximal Humeral Fractures: Is Function Affected by Age, Time, and Fracture Patterns?" ref_num: 82 evidence_tier: paper evidence_level: 4 doi: 10.1007/s11999-011-1935-6 year: 2011 - title: "Osteoporosis does not affect bone mineral density change in the proximal humerus or the functional outcome after open reduction and internal fixation of unilateral displaced 3- or 4-part fractures at 12-month follow-up" ref_num: 91 evidence_tier: paper evidence_level: 1 doi: 10.1016/j.jse.2022.07.008 year: 2023 - title: "Effect of reduced orbital rotation on image quality and intra-articular screw detection in intraoperative 3D imaging of proximal humerus plate fixation: a cadaveric study" ref_num: 92 evidence_tier: paper evidence_level: 5 doi: 10.1186/s13018-026-06800-9 year: 2026 - title: "Acute deep infection after surgical fixation of proximal humeral fractures" ref_num: 93 evidence_tier: paper evidence_level: 4 doi: 10.1016/j.jse.2006.09.021 year: 2007 - title: "Cement-augmented locked plate fixation proximal humerus fractures in elderly patient: a systematic review and meta-analysis" ref_num: 96 evidence_tier: paper evidence_level: 1 doi: 10.1186/s12891-024-07502-1 year: 2024 - title: "Complications of locked plating for proximal humeral fractures—are we getting any better?" ref_num: 97 evidence_tier: paper evidence_level: 4 doi: 10.1016/j.jse.2016.02.015 year: 2016 - title: "In-hospital Complications Are More Likely to Occur After Reverse Shoulder Arthroplasty Than After Locked Plating for Proximal Humeral Fractures" ref_num: 98 evidence_tier: paper evidence_level: 3 doi: 10.1097/corr.0000000000001776 year: 2021 - title: "Factors predicting complication rates after primary shoulder arthroplasty" ref_num: 101 evidence_tier: paper evidence_level: 2 doi: 10.1016/j.jse.2010.11.005 year: 2011 - title: "Morbidity and mortality of fragility proximal humerus fractures: a retrospective cohort study of patients presenting to a level one trauma center" ref_num: 103 evidence_tier: paper evidence_level: 3 doi: 10.1016/j.jse.2022.03.006 year: 2022 - title: "Shoulder Arthrodesis" ref_num: 107 evidence_tier: paper evidence_level: 5 doi: 10.5435/jaaos-d-21-00667 year: 2022 synthesis_version: "v2" verifier_status: skipped
Overview¶
- Locking plate fixation of proximal humerus fractures in patients older than 60 years is associated with a 44% complication rate and a 34% failure rate [1].
- ORIF of nonosteoporotic proximal humeral fractures with locking plates leads to favorable functional and radiologic outcomes at a minimum of 10 years of follow-up [2].
- Nail versus plate fixation of three-part proximal humeral fractures yields similar 1-year outcomes, suggesting both techniques are useful for internal fixation [3].
- Percutaneous treatment of selected proximal humeral fractures results in predictable union and good clinical results with a low rate of complications [5].
- Fixation of proximal humeral fractures with locking plates or locking intramedullary nails produces similar clinical and radiologic results [6].
- The locking plate is an excellent device for managing displaced unstable proximal humeral fractures and expands the indications for ORIF in these fractures [7].
- Distal AO/OTA C-type distal humerus fractures in older adults can be treated reliably with good outcomes using ORIF with modern locking plates [10].
- Locking plates are a good treatment alternative for elderly patients with displaced 2-part fractures of the surgical neck of the proximal humerus, offering acceptable complication rates and functional outcomes, provided rigorous attention is paid to avoid screw penetration [11].
- Patients undergoing ORIF for proximal humerus fracture dislocations have reasonable functional outcomes but relatively high avascular necrosis and reoperation rates [14].
- There are no level 1 studies in the English language literature comparing ORIF with hemiarthroplasty for proximal humeral fractures [17].
- Intramedullary fixation represents an alternative treatment option for proximal humeral fractures with specific fixation and biologic advantages, including reported outcomes comparable with other techniques [18].
- Locking plate fixation appears to provide a good option for the majority of patients with unstable proximal humeral fractures, with good functional outcomes [24].
Anatomy & Pathophysiology¶
- Reverse total shoulder arthroplasty can reliably improve shoulder function, patient satisfaction, and pain levels after failed open reduction and internal fixation of proximal humerus fractures [8].
- Greater tuberosity healing does not impact reverse shoulder arthroplasty biomechanics during abduction or forward flexion [30].
- Greater tuberosity healing affects reverse shoulder arthroplasty biomechanics during external rotation [30].
- Range of motion and strength thresholds can identify subjects with normal shoulder function in the context of proximal humerus fractures [31].
- With minimal and moderate amounts of glenohumeral abduction, glenohumeral joint forces are significantly displaced superiorly when inferior tuberosity placement occurs during hemiarthroplasty for four-part proximal humeral fractures [32].
- The biomechanical literature regarding proximal humerus fracture implants is diverse and heterogeneous [33].
- Biomechanical results regarding the safe distance between humerus shaft fracture and distal locking screws in antegrade nailing require confirmation with clinical studies [34].
- A minimally invasive approach combined with a novel anatomical locking plate provides a biomechanical basis to guide clinical treatment of scapular body fractures [35].
- Modified minimally invasive reduction osteosynthesis system (MIROS) fixation for Neer 2 and 3-Part proximal humeral fractures provides adequate fracture stability and permits early shoulder motion [36].
- Modified minimally invasive reduction osteosynthesis system (MIROS) fixation for Neer 2 and 3-Part proximal humeral fractures yields satisfactory functional and radiologic outcomes with fewer complications [36].
- Shoulder rotational ability is improved by systematically repairing tuberosities around the implant in complex shoulder fractures treated by reverse shoulder arthroplasty, provided their consolidation is anatomic [39].
- The insertion of the deltoid muscle in a 90° abduction position in the scapula plane is recommended for assessing objective strength using the Constant score [42].
- Dominance of the affected shoulder has no influence on functional and quality of life outcomes compared with the nondominant shoulder and should not be used to make treatment decisions [44].
- Reliable bony union and improved shoulder function can be expected with thoughtful surgical planning, appropriate implant choice, and meticulous surgical technique in the management of clavicle nonunion and malunion [45].
- Robot navigation-assisted intramedullary nail treatment for humeral shaft fractures helps surgeons determine the insertion point and proximal opening direction faster and more easily [46].
- Robot navigation-assisted intramedullary nail treatment for humeral shaft fractures shortens surgical time and reduces bleeding [46].
- Robot navigation-assisted intramedullary nail treatment for humeral shaft fractures avoids more intraoperative fluoroscopy [46].
- Robot navigation-assisted intramedullary nail treatment for humeral shaft fractures enables patients to achieve better shoulder functional outcomes [46].
- There is variability in the glenopolar angle with increased AP rotational offset of the shoulder radiograph, revealing inaccuracies even at institutions with established protocols [47].
- The SB suture anchor construct has superior interface contact immediately after fixation in humeral greater tuberosity fracture compared to the DR construct [48].
- The DR suture anchor construct offers better contact performance at all abduction angles with applied force in humeral greater tuberosity fracture compared to the SB construct [48].
- Varus and antecurvatum proximal humerus deformities as small as 15 degrees are associated with statistically significant alterations in glenohumeral joint mechanics in proximal humeral fracture malunion [49].
Classification¶
- The HGLS classification is a reliable method of describing fractures of the proximal humerus compared with the Neer and AO systems [79].
- The Neer fracture classification differentiates function in patients treated with locked plating for unstable proximal humeral fractures [82].
Clinical Presentation¶
- Locking plate fixation of proximal humerus fractures in patients older than 60 years is associated with a 44% complication rate and a 34% failure rate [1].
- Percutaneous treatment of selected proximal humeral fractures results in predictable union and good clinical results with a low rate of complications [5].
- Operative treatment, particularly open reduction and internal fixation, is an independent risk factor for inpatient adverse events and mortality in older-aged patients admitted with an isolated fracture of the proximal humerus [12].
- A majority of patients with proximal humeral fractures undergo non-operative treatment [20].
- Surgical treatment of proximal humerus fractures remains far from straightforward, with unpredictable outcomes where factors associated with poor results include being a woman, four-part fracture dislocation, and absence of metaphyseal head extension [64].
Investigations¶
- Locking plate fixation of proximal humerus fractures in patients older than 60 years is associated with a 44% complication rate and a 34% failure rate [1].
- ORIF of nonosteoporotic proximal humeral fractures with locking plates leads to favorable functional and radiologic outcomes at a minimum of 10 years of follow-up [2].
- Percutaneous treatment of selected proximal humeral fractures results in predictable union and good clinical results with a low rate of complications [5].
- In young, active patients with delayed presentation of complex proximal humeral fractures, ORIF with osteotomy and bone grafting is recommended to preserve the humeral head despite the risk of avascular necrosis, as conservative management yields poor functional outcomes [9].
- Failure of the calcar screw to purchase both the proximal and distal fragments was associated with a significantly higher rate of failure of fixation in the surgical treatment of proximal humeral fractures using a locking plate [16].
- The inherent nature of medial comminution of proximal humeral fracture may lead to inferior radiographic outcomes [76].
- BMD changes appeared swiftly in the proximal humerus after treatment of displaced 3- or 4-part fractures with ORIF, particularly affecting the proximal diaphysis [91].
- Intraoperative 3D imaging with a 160° orbital rotation yields sufficient image quality, enabling the reliable identification of intra-articular screws during plate osteosynthesis of the proximal humerus [92].
Treatment¶
Operative Fixation: Locking Plates¶
- Locking plate fixation of proximal humerus fractures in patients older than 60 years is associated with a 44% complication rate and a 34% failure rate [1].
- ORIF of nonosteoporotic proximal humeral fractures with locking plates leads to favorable functional and radiologic outcomes at a minimum of 10 years of follow-up [2].
- Primary ORIF is supported for medically fit patients with severely displaced fractures or fracture-dislocations of the proximal humerus in centers with appropriate expertise [4].
- Percutaneous treatment of selected proximal humeral fractures results in predictable union, good clinical results, and a low rate of complications [5].
- The locking plate is an excellent device for managing displaced unstable proximal humeral fractures and expands the indications for ORIF in these cases [7].
- Locking plates are a good treatment alternative for elderly patients with displaced 2-part fractures of the surgical neck, offering acceptable complication rates and functional outcomes, provided screw penetration is avoided [11].
- Operative treatment, particularly open reduction and internal fixation, is an independent risk factor for inpatient adverse events and mortality in older-aged patients admitted with an isolated proximal humerus fracture [12].
- Failure of the calcar screw to purchase both the proximal and distal fragments is associated with a significantly higher rate of fixation failure when using locking plates [16].
- Using the Locking Proximal Humerus Plate for all types of proximal humeral fractures is a reliable procedure with good results when careful planning and familiarity with the technique are maintained [19].
- Early results with locked plate fixation are encouraging, providing a potentially viable alternative to prosthetic replacement [23].
- The combined application of medial anatomical locking plate fixation and minimally invasive lateral locking plate fixation is effective in maintaining reduction and preventing varus collapse and implant failure in fractures with an unstable medial column [56].
- The Humerus Block technique is a predictable, minimally invasive, percutaneous operative technique for various proximal humeral fractures that results in good pain relief, mobility, and pull force with a low incidence of avascular necrosis [78].
- Long PHILOS plate fixation provides reliable secure fixation for complex humeral fractures, including long segment periarticular fractures, segmental fractures involving the proximal humerus and shaft, periprosthetic fractures around well-fixed humeral resurfacing prostheses, and pathological fractures [71].
- Dual plating is indicated for certain cases, particularly old ununited fractures where intramedullary nailing is difficult, but is contraindicated in severely comminuted fractures requiring extensive dissection [68].
Operative Fixation: Intramedullary Nails¶
- Fixation of proximal humeral fractures with locking plates or locking intramedullary nails produces similar clinical and radiologic results [6].
- The intramedullary nail is superior to the locking plate in reducing total complications, intraoperative blood loss, operative time, postoperative fracture healing time, and postoperative humeral head necrosis rate [13].
- Intramedullary fixation represents an alternative treatment option with specific fixation and biologic advantages and reported outcomes comparable to other techniques [18].
- Modern proximal humeral nail designs and techniques have demonstrated promising outcomes and can provide stable fixation [70].
Operative Fixation: Other Techniques¶
- Double plate fixation combined with autogenous iliac crest bone grafting results in successful salvage of humeral shaft nonunion after prior failed surgical interventions [15].
- An anterior approach for open reduction and internal fixation of humeral midshaft fractures allows supine positioning and yields union and complication rates comparable to a posterior approach [54].
- The use of a modified anterolateral approach and intra-osseous portal is safe and effective for minimally invasive reduction and plating of three-part proximal humeral fractures [53].
Operative vs. Non-Operative Management¶
- Similar 1-year outcomes for nail versus plate fixation of three-part proximal humeral fractures suggest both techniques are useful for internal fixation [3].
- A majority of patients with proximal humerus fractures undergo non-operative treatment [20].
- Nonsurgical management of proximal humerus fractures decreased during the study period analyzed in one cost-minimization analysis [69].
- There is no significant difference in clinical outcomes at 2 years between surgery and non-operative treatment in patients 60 years of age or older with displaced 2-part fractures of the proximal humerus [59].
- Nonsurgical treatment should have a more prominent role in the treatment of proximal humeral fractures, with better midterm outcomes observed compared to surgical treatment in one study [72].
- Treatment for proximal humerus fractures remains controversial, with nonsurgical management demonstrating successful outcomes and union rates greater than 90% [60].
- Most proximal humeral fractures in elderly patients can be treated nonoperatively with good functional outcomes [73].
- Short and long periods of immobilization yield similar results for nonoperatively treated proximal humeral fractures, independent of the fracture pattern [63].
Perioperative Considerations and Risk Factors¶
- The most important risk factors for postoperative opioid dependence following proximal humerus fractures are preoperative dependence and fracture complexity [80].
Complications¶
- Locking plate fixation of proximal humerus fractures in patients older than 60 years is associated with a 44% complication rate and a 34% failure rate [1].
- ORIF of nonosteoporotic proximal humeral fractures with locking plates leads to favorable functional and radiologic outcomes at a minimum of 10 years of follow-up [2].
- Percutaneous treatment of selected proximal humeral fractures results in a low rate of complications [5].
- Operative treatment, particularly open reduction and internal fixation, is an independent risk factor for inpatient adverse events and mortality in older-aged patients admitted with an isolated fracture of the proximal humerus [12].
- Intramedullary nailing is superior to locking plate fixation in reducing the total complication rate of proximal humerus fractures [13].
- Intramedullary nailing is superior to locking plate fixation in reducing the postoperative humeral head necrosis rate of proximal humerus fractures [13].
- ORIF of proximal humerus fracture dislocations carries a high rate of reoperation [27].
- The incidence of major wound complications after fixation of distal humerus fractures is substantial, with Grade III open fractures and the use of a plate to stabilize the olecranon osteotomy identified as significant risk factors [28].
- Acute deep infection after ORIF of proximal humeral fractures is a devastating complication with high complication rates, poor functional outcomes, and a notably high nonunion rate [93].
- Fixation of proximal humeral fractures in elderly patients using cement-augmented locked plates may result in lesser implant failure and total complication rates compared to using a locked plate alone [96].
- The overall complication rate of locking plate osteosynthesis for proximal humeral fractures has been decreasing considerably within the last years [97].
- In-hospital complications are more likely to occur after reverse shoulder arthroplasty than after locked plating for proximal humeral fractures [98].
- The risk of short-term complications is highest in patients undergoing shoulder arthroplasty for a fracture compared with nonfracture indications [101].
- Mortality at 1 year for fragility proximal humerus fractures is universally high regardless of risk factors [103].
- Complications of shoulder arthrodesis are not uncommon, including nonunion, malunion, fracture, and infection [107].
Recovery¶
- Locking plate fixation of proximal humerus fractures in patients older than 60 years is associated with a 44% complication rate and a 34% failure rate [1].
- ORIF of nonosteoporotic proximal humeral fractures with locking plates leads to favorable functional and radiologic outcomes at a minimum of 10 years of follow-up [2].
- Percutaneous treatment of selected proximal humeral fractures results in predictable union and good clinical results with a low rate of complications [5].
- Shoulder function, patient satisfaction, and pain levels can be reliably improved after reverse total shoulder arthroplasty for failed open reduction and internal fixation of fractures of the proximal humerus [8].
- In young, active patients with delayed presentation of complex proximal humeral fractures, ORIF with osteotomy and bone grafting is recommended to preserve the humeral head, despite the risk of avascular necrosis, as conservative management yields poor functional outcomes [9].
- The intramedullary nail is superior to locking plate in reducing total complication, intraoperative blood loss, operative time, postoperative fracture healing time, and postoperative humeral head necrosis rate of proximal humerus fractures [13].
- Patients undergoing ORIF for proximal humerus fracture dislocations have reasonable functional outcomes but relatively high avascular necrosis and reoperation rates [14].
- Double plate fixation combined with autogenous iliac crest bone grafting results in successful salvage of humeral shaft nonunion after prior failed surgical interventions [15].
- Elective implant removal in symptomatic patients after internal fixation of proximal humerus fractures improves clinical outcome, with symptomatic patients showing statistically significant improvement of the Constant score after implant removal [21].
- Delays beyond 5 days to surgery do not affect outcome following plate and screw fixation of proximal humerus fractures [22].
- ORIF of proximal humerus fracture dislocations carries a high rate of reoperation [27].
- Early active motion rehabilitation for postoperative treatment after locking plate fixation of proximal humerus fractures was not inferior to a restrictive treatment protocol after a follow-up period of 24 months [38].
- Intramedullary stabilization of proximal humeral fractures with an angular and sliding stable antegrade locking nail allows for immediate postoperative mobilization [50].
- Patients with proximal humeral fractures treated with early range of motion exercises do well, largely returning to baseline functional status by 1 year [51].
- Treatment with continuous passive motion (CPM) increases the range of motion after plate osteosynthesis of proximal humerus fractures in the first 6 weeks after surgery, but this effect is not sustained after 3 and 12 months [52].
- External fixation is a preferred surgical treatment option for paediatric proximal humerus fractures because early mobilization of the affected limb can be realized [62].
- The locked plate may prove useful in earlier pain-free rehabilitation of proximal humeral fractures [66].
- Ten years after locked plating of displaced proximal humeral fractures, patients show good to excellent outcomes in the majority of cases with no relevant decline compared with the shoulder function 1 year after surgery [67].
Key Evidence¶
- [L4] ORIF of proximal humerus fractures with locking plates in patients aged >60 years resulted in a 44% complication and 34% failure rate. (10.1016/j.jse.2019.11.026)
- [L3] ORIF of nonosteoporotic proximal humeral fractures with locking plates led to favorable functional and radiologic outcomes at a minimum of 10 years of follow-up. (10.1097/corr.0000000000002895)
- [L2] The similar 1-year outcomes for nail versus plate fixation of three-part proximal humeral fractures suggest that both techniques may be useful for internal fixation of these fractures. (10.1007/s11999-011-2056-y)
- [L4] Our results support the use of primary ORIF in medically fit patients with a severely displaced fracture or a fracture-dislocation of the proximal part of the humerus in centers where the expertise to carry out such treatment exists. (10.2106/jbjs.19.00595)
- [L4] Percutaneous treatment of selected proximal humeral fractures results in predictable union and good clinical results with a low rate of complications. (10.1016/j.jse.2006.09.006)
- [L1] Fixation of proximal humeral fractures with locking plates or locking intramedullary nails produces similar clinical and radiologic results. (10.1016/j.jse.2016.02.003)
- [L2] The locking plate is an excellent device in the management of displaced unstable proximal humeral fractures and is expanding the indications for ORIF in these fractures. (10.1016/j.jse.2009.08.008)
- [L4] Shoulder function, patient satisfaction, and pain levels can be reliably improved. (10.1016/j.jse.2016.05.020)
- [L4] In young, active patients with delayed presentation of complex proximal humeral fractures, ORIF with osteotomy and bone grafting is recommended to preserve the humeral head, despite the risk of avascular necrosis, as conservative management yields poor functional outcomes. (10.1016/j.jse.2007.12.012)
- [L3] Distal AO/OTA C-type distal humerus fractures in older adults can be treated reliably and with good outcomes with ORIF using modern locking plates. (10.1186/s12891-022-05431-5)
- [L4] Locking plates appear to be a good treatment alternative in elderly patients with a displaced 2-part fracture of the surgical neck of the proximal humerus with an acceptable complication rate and an acceptable functional outcome; however, rigorous attention has to be paid to avoid screw penetration. (10.1016/j.jse.2009.11.046)
- [L3] Operative treatment, particularly open reduction and internal fixation, is an independent risk factor for inpatient adverse events and mortality in older-aged patients admitted with an isolated fracture of the proximal humerus and should perhaps be offered more judiciously. (10.1016/j.jse.2013.09.006)
- [L1] The intramedullary nail is superior to locking plate in reducing the total complication, intraoperative blood loss, operative time, postoperative fracture healing time and postoperative humeral head necrosis rate of PHF. (10.1186/s13018-019-1345-0)
- [L4] Patients undergoing ORIF for proximal humerus fracture dislocations have reasonable functional outcomes but relatively high avascular necrosis and reoperation rates. (10.1016/j.jse.2022.04.018)
- [L4] Double plate fixation combined with autogenous iliac crest bone grafting results in successful salvage of humeral shaft nonunion after prior failed surgical interventions. (10.1186/s12891-020-03743-y)
- [L3] Failure of the calcar screw to purchase both the proximal and distal fragments was associated with a significantly higher rate of failure of fixation in the surgical treatment of proximal humeral fractures using a locking plate. (10.1302/0301-620x.107b9.bjj-2024-1649.r1)
- [L5] There are no level 1 studies in the English language literature comparing ORIF with hemiarthroplasty for proximal humeral fractures. (10.1016/j.jhsa.2010.07.019)
- [L4] Intramedullary fixation represents an alternative treatment option for proximal humeral fractures with specific fixation and biologic advantages, including reported outcomes comparable with other techniques. (10.5435/jaaos-d-18-00360)
- [L2] Using the Locking Proximal Humerus Plate for treatment of proximal humeral fractures of all types is a reliable procedure, with good results being obtained with careful planning and familiarity with the special features of the operative technique. (10.1097/01.blo.0000137554.91189.a9)
- [L3] A majority of patients with proximal humeral fractures underwent non-operative treatment. (10.1186/s12891-019-2812-9)
- [L4] Symptomatic patients after locked plate osteosynthesis for proximal humerus fractures showed statistically significant improvement of the Constant score after implant removal. (10.1186/s12891-016-0977-z)
- [L3] Timing of surgery did not impact outcomes of patients who underwent ORIF for proximal humerus fractures. (10.1016/j.jse.2025.02.019)
- [L4] Early results with locked plate fixation for the treatment of proximal humerus fractures have been encouraging, providing a potentially viable alternative to prosthetic replacement. (10.5435/00124635-200805000-00008)
- [L4] Locking plate fixation appears to provide a good option for the majority of patients with unstable proximal humeral fractures, with good functional outcomes. (10.1016/j.jse.2006.06.006)
- [L4] ORIF of proximal humerus fracture dislocations carries a high rate of reoperation. (10.1016/j.jse.2021.01.025)
- [L4] The incidence of major wound complications after fixation of distal humerus fractures is substantial, with Grade III open fractures and the use of a plate to stabilize the olecranon osteotomy identified as significant risk factors. (10.1016/j.jse.2013.09.014)
- [L5] Greater tuberosity healing does not seem to impact reverse shoulder arthroplasty biomechanics during abduction or forward flexion; however, it does affect biomechanics during external rotation. (10.1016/j.jse.2019.07.022)
- [L3] Range of motion and strength thresholds can identify subjects with normal shoulder function. (10.1016/j.jse.2010.06.005)
- [L5] With minimal and moderate amounts of glenohumeral abduction, glenohumeral joint forces are significantly displaced superiorly. (10.1016/j.jse.2007.06.017)
- [L4] The biomechanical literature was found to be both diverse and heterogeneous. (10.1186/s12891-015-0627-x)
- [L5] These biomechanical results, although very promising, should be confirmed with clinical studies. (10.1186/s12891-025-08711-y)
- [L5] The study provided a biomechanical basis to guide the clinical treatment of scapular body fractures. (10.1186/s13018-024-04905-7)
- [L3] It is a minimally invasive procedure that provides adequate fracture stability and permits early shoulder motion, with satisfactory functional and radiologic outcomes and fewer complications. (10.1186/s12891-025-08600-4)
- [L2] Early active motion rehabilitation for postoperative treatment after locking plate fixation of proximal humerus fractures was not inferior to a restrictive treatment protocol after a follow-up period of 24 months. (10.1016/j.jse.2025.01.042)
- [L3] Shoulder rotational ability is improved by systematically repairing the tuberosities around the implant, provided their consolidation is anatomic. (10.1016/j.jse.2012.03.011)
- [L3] The authors recommend performing the measurement at the insertion of the deltoid muscle in a 90° abduction position in the scapula plane. (10.1186/s12891-019-2795-6)
- [L3] Dominance of the affected shoulder has no influence and should not be used to make treatment decisions. (10.1016/j.jse.2014.10.006)
- [L5] Reliable bony union and improved shoulder function can be expected with thoughtful surgical planning, appropriate implant choice, and meticulous surgical technique. (10.1016/j.jse.2013.01.022)
- [L3] It can help surgeons determine the insertion point and proximal opening direction faster and more easily, shorten the surgical time, reduce bleeding, avoid more intraoperative fluoroscopy, and enable patients to achieve better shoulder functional outcomes. (10.1186/s12891-024-07848-6)
- [L4] The study demonstrates variability in the glenopolar angle with increased AP rotational offset of the shoulder radiograph, revealing inaccuracies even at an institution with an established protocol. (10.1302/0301-620x.95b8.30631)
- [L5] Findings suggest that despite the SB construct having superior interface contact immediately after fixation, the DR construct offered better contact performance at all abduction angles with applied force. (10.1186/s12891-019-2412-8)
- [L5] Varus and antecurvatum proximal humerus deformities as small as 15 degrees were associated with statistically significant alterations in glenohumeral joint mechanics. (10.5435/jaaos-d-20-00555)
- [L4] Intramedullary stabilization of proximal humeral fractures with an angular and sliding stable antegrade locking nail represents a minimally invasive procedure that provides a high degree of primary stability even in osteoporotic bone and allows for immediate postoperative mobilization. (10.2106/00004623-200300004-00019)
- [L3] Patients with proximal humeral fractures treated with early range of motion exercises do well, largely returning to baseline functional status by 1 year. (10.1016/j.jse.2007.07.016)
- [L1] The treatment with CPM increases the range of motion after plate osteosynthesis of proximal humerus fractures in the first 6 weeks after surgery, but this effect is not sustained after 3 and 12 months. (10.1186/s13018-024-04804-x)
- [L3] The use of the modified anterolateral approach and intra-osseous portal is safe and effective for minimally invasive reduction and plating treatment for three-part proximal humeral fractures. (10.1186/s13018-017-0701-1)
- [L3] An anterior approach allows supine positioning of the patient and yields union and complication rates comparable to those of a posterior approach with plate fixation for the treatment of humeral shaft fractures. (10.1186/s12891-019-2888-2)
- [L4] The combined application of medial anatomical locking plate fixation and minimally invasive lateral locking plate fixation is effective in maintaining operative reduction and preventing varus collapse and implant failure in proximal humerus fractures with an unstable medial column. (10.1186/s13018-020-02094-7)
- [L1] This trial found no significant difference in clinical outcomes at 2 years between surgery and non-operative treatment in patients 60 years of age or older with displaced 2-part fractures of the proximal humerus. (10.1371/journal.pmed.1002855)
- [L5] Treatment for proximal humerus fractures remains controversial, with nonsurgical management demonstrating successful outcomes and union rates greater than 90%. (10.5435/jaaos-d-24-01073)
- [L3] External fixation is a preferred surgical treatment option for paediatric proximal humerus fractures because early mobilization of the affected limb can be realized. (10.1186/s12891-023-07037-x)
- [L2] Short and long periods of immobilization yield similar results for nonoperatively treated proximal humeral fractures, independent of the fracture pattern. (10.2106/jbjs.20.02137)
- [L5] Surgical treatment of proximal humerus fractures remains far from straightforward, with unpredictable outcomes where factors associated with poor results include being a woman, four-part fracture dislocation, and absence of metaphyseal head extension. (10.1097/corr.0000000000002242)
- [L5] The locked plate may prove useful in earlier pain-free rehabilitation of proximal humeral fractures. (10.1016/j.jse.2006.03.013)
- [L4] Ten years after locked plating of displaced proximal humeral fractures, patients show good to excellent outcomes in the majority of cases with no relevant decline compared with the shoulder function 1 year after surgery. (10.1016/j.jse.2013.11.009)
- [L4] Dual plating is still indicated for certain cases, particularly old ununited fractures where intramedullary nailing is difficult, but is contraindicated in severely comminuted fractures requiring extensive dissection. (10.2106/00004623-196345020-00026)
- [L4] Nonsurgical management of proximal humerus fractures decreased during the study period. (10.1016/j.jhsa.2020.03.022)
- [L5] Modern proximal humeral nail designs and techniques have demonstrated promising outcomes and can provide stable fixation. (10.1016/j.jse.2015.11.016)
- [L4] The long PHILOS plate fixation provides reliable secure fixation for the treatment of complex humeral fractures, especially long segment periarticular fractures, segmental fractures involving proximal humerus and shaft, periprosthetic fractures around well-fixed humeral resurfacing prosthesis and pathological fractures. (10.1111/j.1758-5740.2010.00085.x)
- [L3] Nonsurgical treatment should have a more prominent role in the treatment of proximal humeral fractures. (10.1016/j.jse.2011.01.025)
- [L5] Most proximal humeral fractures in elderly patients can be treated nonoperatively with good functional outcomes. (10.2106/jbjs.l.01293)
- [L3] This implies that the inherent nature of medial comminution of proximal humeral fracture may lead to inferior radiographic outcomes. (10.1186/s13018-022-03337-5)
- [L4] The Humerus Block technique is a very good and predictable, minimally invasive, percutaneous operative technique for treatment of various types of proximal humeral fractures that results in very good pain relief, mobility, and pull force in the arm with a low incidence of avascular necrosis. (10.1016/j.jse.2011.07.029)
- [L3] The HGLS classification is a reliable method of describing fractures of the proximal humerus compared with the Neer and AO systems. (10.1016/j.jse.2012.09.018)
- [L3] The most important risk factors for postoperative opioid dependence following proximal humerus fractures are preoperative dependence and fracture complexity. (10.1186/s13018-019-1233-7)
- [L4] With locked plating of unstable proximal humeral fractures, older patients function as well as younger patients; improvement continues until 1 year postoperatively, the Neer fracture classification differentiates function, and polytrauma patients perform worse clinically. (10.1007/s11999-011-1935-6)
- [L1] BMD changes appeared swiftly in the proximal humerus after treatment of displaced 3- or 4-part fractures with ORIF, particularly affecting the proximal diaphysis. (10.1016/j.jse.2022.07.008)
- [L5] Intraoperative 3D imaging with a 160° orbital rotation yields sufficient image quality, enabling the reliable identification of intra-articular screws during plate osteosynthesis of the proximal humerus. (10.1186/s13018-026-06800-9)
- [L4] Acute deep infection after ORIF of proximal humeral fractures is a devastating complication with high complication rates, poor functional outcomes, and a notably high nonunion rate. (10.1016/j.jse.2006.09.021)
- [L1] Fixation of proximal humeral fractures in elderly patients using locked plates with or without cement augmentation has no significant difference in revision rate, but the implant failure and total complication rates may be lesser on using the cement-augmented locked plate for fixation than on using a locked plate alone. (10.1186/s12891-024-07502-1)
- [L4] The overall complication rate of locking plate osteosynthesis for proximal humeral fractures has been decreasing considerably within the last years. (10.1016/j.jse.2016.02.015)
- [L3] The increased in-hospital risk for major adverse events and surgical complications may moderate the enthusiasm associated with RTSA for proximal humeral fractures in patients 65 years and older. (10.1097/corr.0000000000001776)
- [L2] The findings indicate that the risk of short-term complications is highest in patients undergoing surgery for a fracture compared with nonfracture indications. (10.1016/j.jse.2010.11.005)
- [L3] Mortality at 1 year for fragility proximal humerus fractures is universally high regardless of risk factors. (10.1016/j.jse.2022.03.006)
- [L5] Complications are not uncommon, including nonunion, malunion, fracture, and infection. (10.5435/jaaos-d-21-00667)
References¶
[1] Locking plate fixation of proximal humerus fractures in patients older than 60 years continues to be associated with a high complication rate. Journal of Shoulder and Elbow Surgery. 2020. DOI: 10.1016/j.jse.2019.11.026 [2] What Are the Long-term Outcomes of Locking Plates for Nonosteoporotic Three-part and Four-part Proximal Humeral Fractures With a Minimum 10-year Follow-up Period?. Clinical Orthopaedics & Related Research. 2023. DOI: 10.1097/corr.0000000000002895 [3] Similar Outcomes for Nail versus Plate Fixation of Three-part Proximal Humeral Fractures. Clinical Orthopaedics & Related Research. 2012. DOI: 10.1007/s11999-011-2056-y [4] Complications and Long-Term Outcomes of Open Reduction and Plate Fixation of Proximal Humeral Fractures. Journal of Bone and Joint Surgery. 2019. DOI: 10.2106/jbjs.19.00595 [5] Outcomes after percutaneous reduction and fixation of proximal humeral fractures. Journal of Shoulder and Elbow Surgery. 2007. DOI: 10.1016/j.jse.2006.09.006 [6] Locking intramedullary nails compared with locking plates for two- and three-part proximal humeral surgical neck fractures: a randomized controlled trial. Journal of Shoulder and Elbow Surgery. 2016. DOI: 10.1016/j.jse.2016.02.003 [7] The results of ORIF of displaced unstable proximal humeral fractures using a locking plate. Journal of Shoulder and Elbow Surgery. 2010. DOI: 10.1016/j.jse.2009.08.008 [8] Reverse total shoulder arthroplasty for failed open reduction and internal fixation of fractures of the proximal humerus. Journal of Shoulder and Elbow Surgery. 2017. DOI: 10.1016/j.jse.2016.05.020 [9] Four-part valgus impacted proximal humeral fracture presenting three months after injury in a young patient: Open reduction and internal fixation with triple osteotomy and bone graft augmentation. Journal of Shoulder and Elbow Surgery. 2009. DOI: 10.1016/j.jse.2007.12.012 [10] Outcomes of AO/OTA C-type fractures of the distal humerus after open reduction and internal fixation with locking plate constructs in patients at least 65 years old. BMC Musculoskeletal Disorders. 2022. DOI: 10.1186/s12891-022-05431-5 [11] Quality of life and functional outcome after a 2-part proximal humeral fracture: A prospective cohort study on 50 patients treated with a locking plate. Journal of Shoulder and Elbow Surgery. 2010. DOI: 10.1016/j.jse.2009.11.046 [12] Treatment choice affects inpatient adverse events and mortality in older aged inpatients with an isolated fracture of the proximal humerus. Journal of Shoulder and Elbow Surgery. 2014. DOI: 10.1016/j.jse.2013.09.006 [13] Effect of intramedullary nail and locking plate in the treatment of proximal humerus fracture: an update systematic review and meta-analysis. Journal of Orthopaedic Surgery and Research. 2019. DOI: 10.1186/s13018-019-1345-0 [14] Fracture dislocations of the proximal humerus treated with open reduction and internal fixation: a systematic review. Journal of Shoulder and Elbow Surgery. 2022. DOI: 10.1016/j.jse.2022.04.018 [15] Double plating with autogenous bone grafting as a salvage procedure for recalcitrant humeral shaft nonunion. BMC Musculoskeletal Disorders. 2020. DOI: 10.1186/s12891-020-03743-y [16] Purchase of both proximal and distal fragments by the calcar screw is critical when using a locking plate in the treatment of proximal humeral fractures. The Bone & Joint Journal. 2025. DOI: 10.1302/0301-620x.107b9.bjj-2024-1649.r1 [17] Three- and Four-Part Proximal Humerus Fractures: Open Reduction and Internal Fixation Versus Arthroplasty. The Journal of Hand Surgery. 2010. DOI: 10.1016/j.jhsa.2010.07.019 [18] Intramedullary Fixation for Proximal Humeral Fractures. Journal of the American Academy of Orthopaedic Surgeons. 2020. DOI: 10.5435/jaaos-d-18-00360 [19] A New Locking Plate for Unstable Fractures of the Proximal Humerus. Clinical Orthopaedics & Related Research. 2005. DOI: 10.1097/01.blo.0000137554.91189.a9 [20] Readmissions, revisions, and mortality after treatment for proximal humeral fractures in three large states. BMC Musculoskeletal Disorders. 2019. DOI: 10.1186/s12891-019-2812-9 [21] Elective implant removal in symptomatic patients after internal fixation of proximal humerus fractures improves clinical outcome. BMC Musculoskeletal Disorders. 2016. DOI: 10.1186/s12891-016-0977-z [22] Delays beyond 5 days to surgery does not affect outcome following plate and screw fixation of proximal humerus fractures. Journal of Shoulder and Elbow Surgery. 2025. DOI: 10.1016/j.jse.2025.02.019 [23] Fixed-angle Locked Plating of Two-, Three-, and Four-part Proximal Humerus Fractures. Journal of the American Academy of Orthopaedic Surgeons. 2008. DOI: 10.5435/00124635-200805000-00008 [24] Locking plate fixation for proximal humeral fractures: Initial results with a new implant. Journal of Shoulder and Elbow Surgery. 2007. DOI: 10.1016/j.jse.2006.06.006 [27] Outcomes of open reduction and internal fixation of proximal humerus fracture dislocations. Journal of Shoulder and Elbow Surgery. 2021. DOI: 10.1016/j.jse.2021.01.025 [28] Wound complications after distal humerus fracture fixation: incidence, risk factors, and outcome. Journal of Shoulder and Elbow Surgery. 2014. DOI: 10.1016/j.jse.2013.09.014 [30] The role of greater tuberosity healing in reverse shoulder arthroplasty: a finite element analysis. Journal of Shoulder and Elbow Surgery. 2020. DOI: 10.1016/j.jse.2019.07.022 [31] Does objective shoulder impairment explain patient-reported functional outcome? A study of proximal humerus fractures. Journal of Shoulder and Elbow Surgery. 2011. DOI: 10.1016/j.jse.2010.06.005 [32] Neer Award 2006: Biomechanical assessment of inferior tuberosity placement during hemiarthroplasty for four-part proximal humeral fractures. Journal of Shoulder and Elbow Surgery. 2008. DOI: 10.1016/j.jse.2007.06.017 [33] A scoping review of biomechanical testing for proximal humerus fracture implants. BMC Musculoskeletal Disorders. 2015. DOI: 10.1186/s12891-015-0627-x [34] Mechanical study of the safe distance between humerus shaft fracture and distal locking screws in antegrade nailing. BMC Musculoskeletal Disorders. 2025. DOI: 10.1186/s12891-025-08711-y [35] Finite element analysis of the treatment of a minimally invasive approach combined with a novel anatomical locking plate for scapular body fractures. Journal of Orthopaedic Surgery and Research. 2024. DOI: 10.1186/s13018-024-04905-7 [36] Assessment of fracture stability following modified minimally invasive reduction osteosynthesis system (MIROS) fixation for Neer 2 and 3-Part proximal humeral fractures. BMC Musculoskeletal Disorders. 2025. DOI: 10.1186/s12891-025-08600-4 [38] Postoperative treatment of proximal humerus fractures with an early active motion protocol: a prospective randomized controlled trail. Journal of Shoulder and Elbow Surgery. 2025. DOI: 10.1016/j.jse.2025.01.042 [39] Improvement in shoulder rotation in complex shoulder fractures treated by reverse shoulder arthroplasty. Journal of Shoulder and Elbow Surgery. 2013. DOI: 10.1016/j.jse.2012.03.011 [42] Evaluation of the Constant score: which is the method to assess the objective strength?. BMC Musculoskeletal Disorders. 2019. DOI: 10.1186/s12891-019-2795-6 [44] Does fracture of the dominant shoulder have any effect on functional and quality of life outcome compared with the nondominant shoulder?. Journal of Shoulder and Elbow Surgery. 2015. DOI: 10.1016/j.jse.2014.10.006 [45] Management of clavicle nonunion and malunion. Journal of Shoulder and Elbow Surgery. 2013. DOI: 10.1016/j.jse.2013.01.022 [46] A clinical study on robot navigationassisted intramedullary nail treatment for humeral shaft fractures. BMC Musculoskeletal Disorders. 2024. DOI: 10.1186/s12891-024-07848-6 [47] The assessment of scapular radiographs. The Bone & Joint Journal. 2013. DOI: 10.1302/0301-620x.95b8.30631 [48] Different suture anchor fixation techniques affect contact properties in humeral greater tuberosity fracture: a biomechanical study. BMC Musculoskeletal Disorders. 2019. DOI: 10.1186/s12891-019-2412-8 [49] Altered Glenohumeral Biomechanics in Proximal Humeral Fracture Malunion. Journal of the American Academy of Orthopaedic Surgeons. 2020. DOI: 10.5435/jaaos-d-20-00555 [50] STABILIZATION OF PROXIMAL HUMERAL FRACTURES WITH AN ANGULAR AND SLIDING STABLE ANTEGRADE LOCKING NAIL (TARGON PH). The Journal of Bone and Joint Surgery-American Volume. 2003. DOI: 10.2106/00004623-200300004-00019 [51] Functional outcome following one-part proximal humeral fractures: A prospective study. Journal of Shoulder and Elbow Surgery. 2008. DOI: 10.1016/j.jse.2007.07.016 [52] Early functional improvements using continuous passive motion therapy after angular-stable plate osteosynthesis of proximal humerus fractures – results of a prospective, randomized trial. Journal of Orthopaedic Surgery and Research. 2024. DOI: 10.1186/s13018-024-04804-x [53] Modified minimally invasive approach and intra-osseous portal for three-part proximal humeral fractures: a comparative study. Journal of Orthopaedic Surgery and Research. 2018. DOI: 10.1186/s13018-017-0701-1 [54] Open reduction and internal fixation of humeral midshaft fractures: anterior versus posterior plate fixation. BMC Musculoskeletal Disorders. 2019. DOI: 10.1186/s12891-019-2888-2 [56] A novel surgical approach and technique and short-term clinical efficacy for the treatment of proximal humerus fractures with the combined use of medial anatomical locking plate fixation and minimally invasive lateral locking plate fixation. Journal of Orthopaedic Surgery and Research. 2021. DOI: 10.1186/s13018-020-02094-7 [59] Operative versus non-operative treatment for 2-part proximal humerus fracture: A multicenter randomized controlled trial. PLOS Medicine. 2019. DOI: 10.1371/journal.pmed.1002855 [60] Contemporary Management of Proximal Humeral Fractures. Journal of the American Academy of Orthopaedic Surgeons. 2025. DOI: 10.5435/jaaos-d-24-01073 [62] Kirschner wire versus external fixation in the treatment of proximal humeral fractures in older children and adolescents: a comparative study. BMC Musculoskeletal Disorders. 2023. DOI: 10.1186/s12891-023-07037-x [63] One Versus 3-Week Immobilization Period for Nonoperatively Treated Proximal Humeral Fractures. Journal of Bone and Joint Surgery. 2021. DOI: 10.2106/jbjs.20.02137 [64] CORR Insights®: What Factors Are Associated With Poor Shoulder Function and Serious Complications After Internal Fixation of Three-part and Four-part Proximal Humerus Fracture-dislocations?. Clinical Orthopaedics & Related Research. 2022. DOI: 10.1097/corr.0000000000002242 [66] Biomechanical evaluation of locked plating in proximal humeral fractures. Journal of Shoulder and Elbow Surgery. 2007. DOI: 10.1016/j.jse.2006.03.013 [67] Long-term functional outcomes (median 10 years) after locked plating for displaced fractures of the proximal humerus. Journal of Shoulder and Elbow Surgery. 2014. DOI: 10.1016/j.jse.2013.11.009 [68] DUAL SLOTTED PLATES IN FIXATION OF FRACTURES OF THE FEMORAL SHAFT. The Journal of Bone & Joint Surgery. 1963. DOI: 10.2106/00004623-196345020-00026 [69] Cost-Minimization Analysis and Treatment Trends of Surgical and Nonsurgical Treatment of Proximal Humerus Fractures. The Journal of Hand Surgery. 2020. DOI: 10.1016/j.jhsa.2020.03.022 [70] Intramedullary nailing of the proximal humerus: evolution, technique, and results. Journal of Shoulder and Elbow Surgery. 2016. DOI: 10.1016/j.jse.2015.11.016 [71] Long Philos Plate Fixation for Complex Humeral Fractures. Shoulder & Elbow. 2010. DOI: 10.1111/j.1758-5740.2010.00085.x [72] Locking plate versus nonsurgical treatment for proximal humeral fractures: better midterm outcome with nonsurgical treatment. Journal of Shoulder and Elbow Surgery. 2011. DOI: 10.1016/j.jse.2011.01.025 [73] Proximal Humeral Fracture Treatment in Adults. Journal of Bone and Joint Surgery. 2014. DOI: 10.2106/jbjs.l.01293 [76] The effect of medial calcar support on proximal humeral fractures treated with locking plates. Journal of Orthopaedic Surgery and Research. 2022. DOI: 10.1186/s13018-022-03337-5 [78] Functional and radiographic medium-term outcome evaluation of the Humerus Block, a minimally invasive operative technique for proximal humeral fractures. Journal of Shoulder and Elbow Surgery. 2012. DOI: 10.1016/j.jse.2011.07.029 [79] A comprehensive classification of proximal humeral fractures: HGLS system. Journal of Shoulder and Elbow Surgery. 2013. DOI: 10.1016/j.jse.2012.09.018 [80] Can patient and fracture factors predict opioid dependence following upper extremity fractures?: a retrospective review. Journal of Orthopaedic Surgery and Research. 2019. DOI: 10.1186/s13018-019-1233-7 [82] Locked Plating of Proximal Humeral Fractures: Is Function Affected by Age, Time, and Fracture Patterns?. Clinical Orthopaedics & Related Research. 2011. DOI: 10.1007/s11999-011-1935-6 [91] Osteoporosis does not affect bone mineral density change in the proximal humerus or the functional outcome after open reduction and internal fixation of unilateral displaced 3- or 4-part fractures at 12-month follow-up. Journal of Shoulder and Elbow Surgery. 2023. DOI: 10.1016/j.jse.2022.07.008 [92] Effect of reduced orbital rotation on image quality and intra-articular screw detection in intraoperative 3D imaging of proximal humerus plate fixation: a cadaveric study. Journal of Orthopaedic Surgery and Research. 2026. DOI: 10.1186/s13018-026-06800-9 [93] Acute deep infection after surgical fixation of proximal humeral fractures. Journal of Shoulder and Elbow Surgery. 2007. DOI: 10.1016/j.jse.2006.09.021 [96] Cement-augmented locked plate fixation proximal humerus fractures in elderly patient: a systematic review and meta-analysis. BMC Musculoskeletal Disorders. 2024. DOI: 10.1186/s12891-024-07502-1 [97] Complications of locked plating for proximal humeral fractures—are we getting any better?. Journal of Shoulder and Elbow Surgery. 2016. DOI: 10.1016/j.jse.2016.02.015 [98] In-hospital Complications Are More Likely to Occur After Reverse Shoulder Arthroplasty Than After Locked Plating for Proximal Humeral Fractures. Clinical Orthopaedics & Related Research. 2021. DOI: 10.1097/corr.0000000000001776 [101] Factors predicting complication rates after primary shoulder arthroplasty. Journal of Shoulder and Elbow Surgery. 2011. DOI: 10.1016/j.jse.2010.11.005 [103] Morbidity and mortality of fragility proximal humerus fractures: a retrospective cohort study of patients presenting to a level one trauma center. Journal of Shoulder and Elbow Surgery. 2022. DOI: 10.1016/j.jse.2022.03.006 [107] Shoulder Arthrodesis. Journal of the American Academy of Orthopaedic Surgeons. 2022. DOI: 10.5435/jaaos-d-21-00667