Proximal Humerus Fixation (ORIF) PDF Evidence¶
Rehabilitation after locking-plate fixation of a proximal humerus fracture, gated on radiographic healing at review.
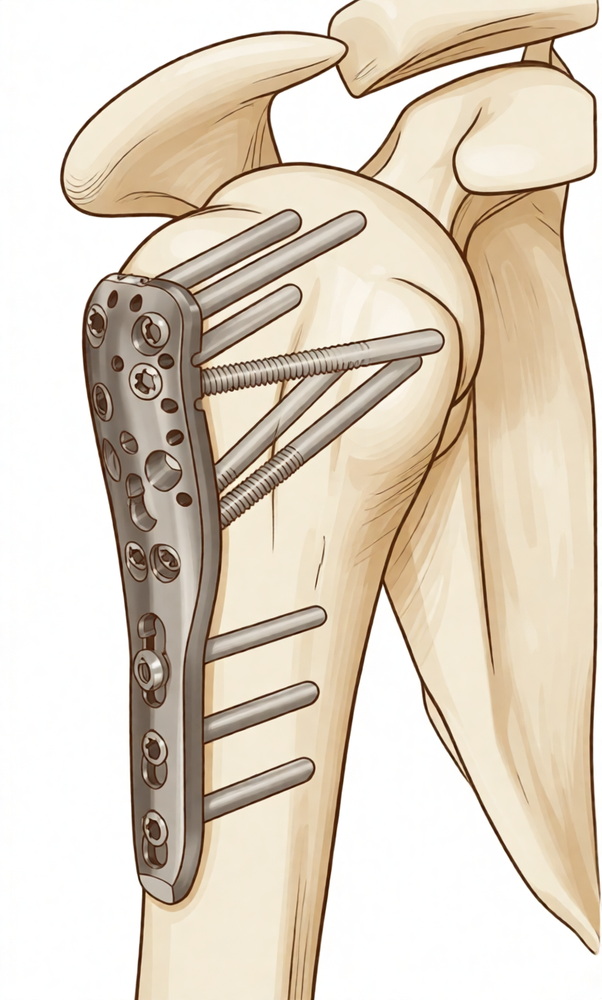
This protocol covers the rehabilitation after surgical fixation of a proximal humerus fracture — a break of the upper arm bone near the shoulder, repaired with a locking plate and screws (open reduction and internal fixation, ORIF) — with Dr Kieran Hirpara at Mater Private Hospital Rockhampton. Bring this page or its PDF to your first physiotherapy visit so your rehabilitation stays coordinated. Your rehabilitation is progressed individually by your physiotherapist through the phases below, depending on how your fracture heals.
If you have any concerns about your wound after surgery, get in touch with the rooms. It is often helpful to take a photo of the wound and email it for review.
What to expect¶
Rehabilitation after a fracture fixation works differently from rehabilitation after most planned shoulder operations. The plate and screws hold the broken bone in position, but the bone itself still has to heal — and the speed of that healing varies considerably from person to person. For that reason, the timetable below is a typical guide rather than a fixed schedule: each step up in your program depends on both the number of weeks since surgery and on how the fracture is healing on your X-rays, as confirmed at your reviews with Dr Hirpara. Do not move yourself on to the next phase on the calendar alone — wait for your review.
There is one more thing that makes this operation different. The bony knobs at the top of the humerus (the tuberosities) are where the rotator cuff tendons attach, and in many proximal humerus fractures these fragments are part of the break and are fixed back with the plate or with stitches. Working the rotator cuff muscles too hard, too early can pull on those fragments before they have healed. With a modern locking plate the fixation is strong from day one, so gentle early movement is encouraged — you may move the shoulder actively-assisted and gently actively within comfort from early on, raising the arm in a pain-free range. The cautious element is rotator-cuff loading: where the tuberosity fragments are not part of the fracture, or are solidly fixed, your surgeon may clear you to begin active rotation and cuff work sooner; where the tuberosities are involved and healing, active rotator-cuff work and forced outward rotation are held back a little longer. Dr Hirpara will tell you which applies to you.
Your exercise program uses three kinds of movement, and your team will mark which apply to you:
- Active range of motion — movement is allowed without aid or help.
- Active-assisted range of motion — using the other arm or an object to assist with moving the arm.
- Passive range of motion — completely relaxed, using the other arm or force to do 100% of the work.
You will wake from surgery with your arm in a sling. Wear it full-time for the first three weeks or so, then wean out of it over the following weeks as comfort allows — published protocols average around three weeks of immobilisation, and the evidence supports earlier movement over longer time in the sling. You don't need to sleep in it. Take it off several times a day for your exercises and for washing and dressing, and when sitting quietly at home you may rest the arm out of the sling. Do not drive while you are wearing the sling.
The journey at a glance:
- Phase I — Protection and early passive movement — weeks 0–6
- Phase II — Regaining active movement — weeks 6–12
- Phase III — Strengthening — about months 3 to 4½
- Phase IV — Return to full activity — from about 4½–6 months
Phase I — Protection and early passive movement (Weeks 0–6)¶
Kieran Hirpara 4.0
Pendulum exercises
Lean forward, supporting yourself on a table with your other hand, and let the operated arm hang relaxed. Make small circles — clockwise, then anticlockwise — by gently rocking your body. The arm swings passively; the movement comes from your body, not the shoulder muscles.
Several times a day
Kieran Hirpara 4.0
Active elbow bends
With the arm out of the sling and the upper arm resting by your side, bend the elbow as far as it will comfortably go, then straighten it fully. Only the elbow moves — keep the shoulder still and the arm by your side.
Several times a day
Kieran Hirpara 4.0
Ball squeezes
With the arm supported, squeeze a soft ball or make a tight fist, then open the hand fully. Keep the fingers, wrist and hand moving each time the arm is out of the sling.
Several times a day
Kieran Hirpara 4.0
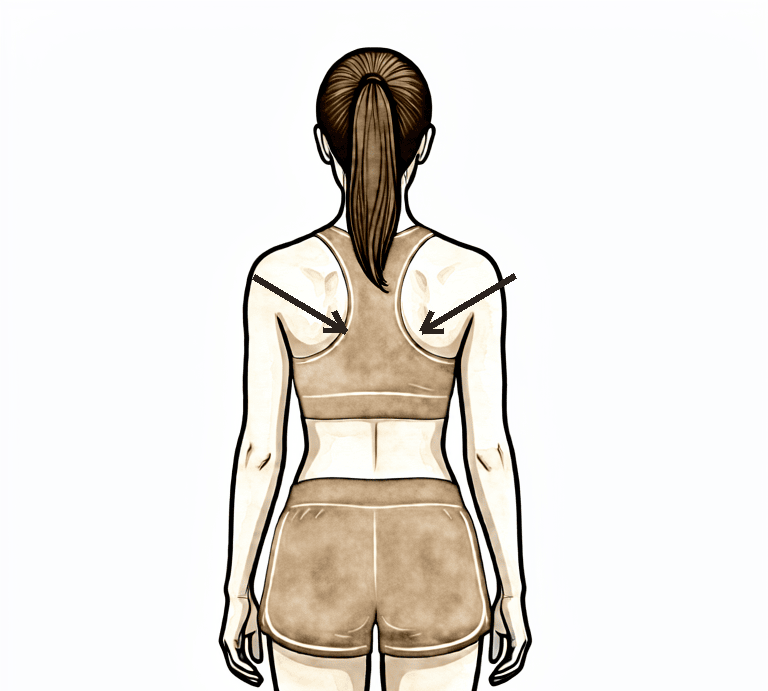
Scapular setting
Sitting or standing tall, gently draw your shoulder blades down and back together without moving the arms, hold for a few seconds, then relax. Keep your ears, shoulders and hips in line.
As guided by your physiotherapist
Kieran Hirpara 4.0
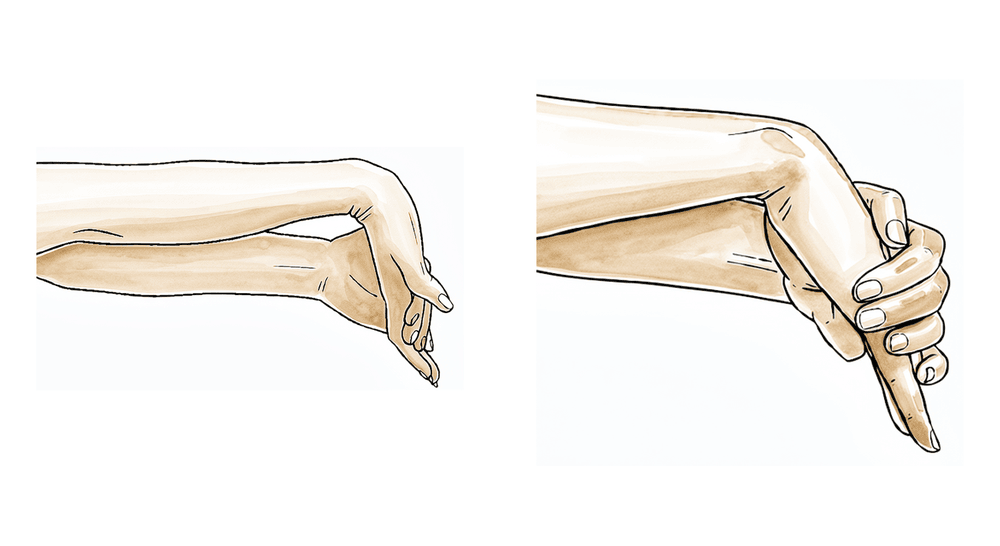
Wrist movements
With the arm out of the sling, keep the wrist moving by bending it forwards, backwards and gently side to side. This keeps the whole arm working while the shoulder is protected.
Several times a day
Kieran Hirpara 4.0
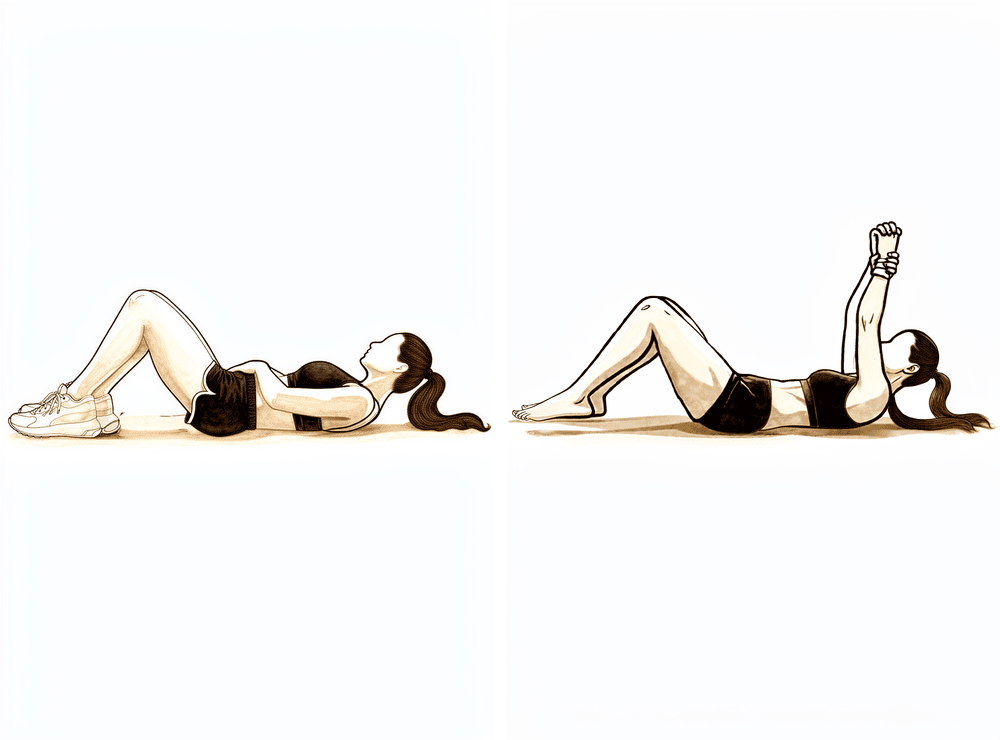
Assisted forward elevation (lying)
Lie on your back and use your good arm to help raise the operated arm up in front of you, then lower it gently with the good arm still helping. Starting on your back lets gravity help and makes early lifting easier. Keep within a comfortable, pain-free range and stop where it begins to pull — do not force it.
Several times a day, within a pain-free range
Kieran Hirpara 4.0
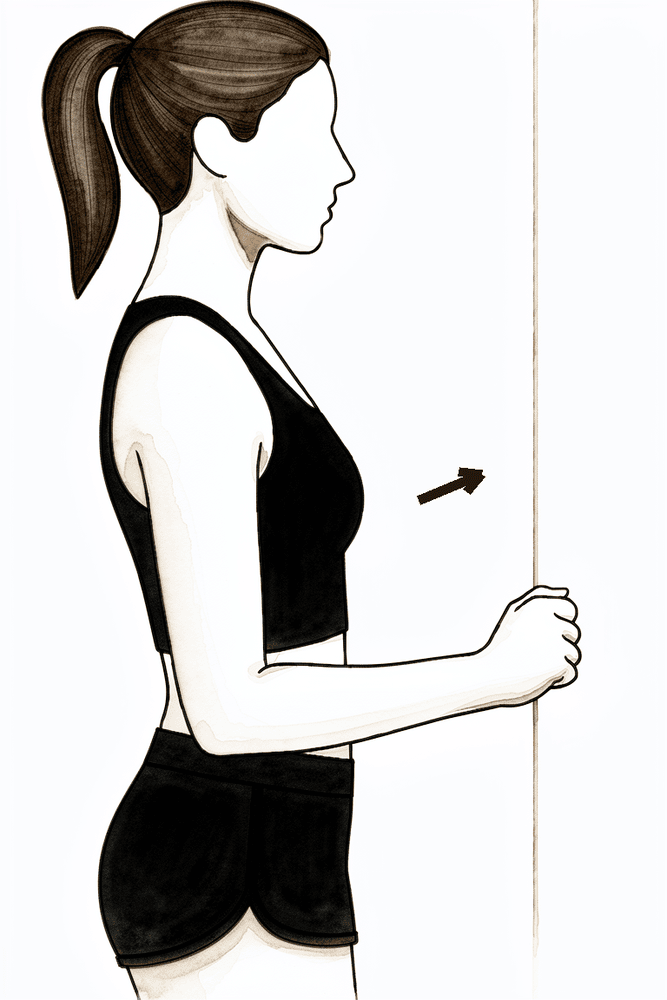
Gentle forward-elevation isometric
Stand facing a wall with the operated arm by your side and a soft fist against the wall in front of you. Gently press the hand forwards into the wall without letting the arm move, hold for a few seconds, then relax. This wakes up the shoulder-lifting muscles without straining the healing fracture. Only if your physiotherapist has started you on it.
As guided by your physiotherapist
The first six weeks are about protecting the fixed fracture while keeping the rest of the arm — and the shoulder joint itself — from stiffening. Because the locking plate holds the bone securely from the start, gentle early movement is encouraged rather than waiting six weeks. A physiotherapist will start you on gentle exercises before you go home: pendulum exercises (letting the arm hang and swing gently by rocking your body), and keeping the elbow, wrist and hand moving out of the sling several times a day. From early on, and within a comfortable, pain-free range, you can begin to move the arm with help from your other hand (active-assisted) and gently under its own power (active) — raising it in front of you as comfort allows. The cautious part is rotator-cuff loading: avoid forcing the arm outwards (external rotation) and avoid resisted rotator-cuff work until your tuberosities have healed, as Dr Hirpara confirms. Use ice for pain relief, and take your painkillers before your exercises and physiotherapy appointments.
For your physiotherapist:
Goals
- Protect the fixation and optimise bony healing
- Settle pain and swelling
- Establish early active-assisted progressing to active elevation within a pain-free range
- Maintain full motion of the neck, elbow, wrist and hand
Management
- Sling full-time for ~3 weeks, then weaned as comfort allows (literature convention); removed several times daily for exercises and hygiene; not required in bed
- Pendulum / Codman exercises several times daily
- Early active-assisted and gentle active forward elevation within a comfortable, pain-free range from the outset for stable fixation — supine-start elevation progressing toward upright as control allows; advance the range as comfort permits
- Passive range of motion as needed where active is not yet tolerated: forward elevation in the scapular plane to about 90°, internal rotation to the belly (not behind the back)
- External rotation kept to a gentle early default of about 30–40° with the arm at the side; the surgeon may advance this where the tuberosities are uninvolved or solidly fixed
- Cervical, elbow, wrist and hand active range of motion out of the sling; ball squeezes for grip
- Scapular setting and scapular mobility work (elevation, depression, retraction, protraction)
- Gentle deltoid and periscapular isometrics may be introduced as comfort allows
- Cryotherapy and analgesia before sessions; scar mobilisation and desensitisation once the wound has healed
Precautions
- Avoid forced or resisted external rotation and heavy rotator-cuff loading until tuberosity healing is confirmed — surgeon-guided; active elevation in a pain-free range is permitted
- No internal rotation behind the back; avoid abduction in the coronal plane
- Keep early movement pain-free — gentle and within comfort, not forced
- No lifting greater than about 0.5–1 kg with the operated arm
- No weight-bearing through the operated arm (no pushing up from a chair or bed)
- No driving while wearing the sling
- No forced or painful end-range movement
Criteria to progress
- Radiographic evidence of healing progressing, as confirmed at the review with Dr Hirpara at about 6 weeks
- Pain well controlled
- Full elbow, wrist and hand motion maintained
- Comfortable active-assisted to active elevation within a pain-free range
Phase II — Regaining active movement (Weeks 6–12)¶
Kieran Hirpara 4.0
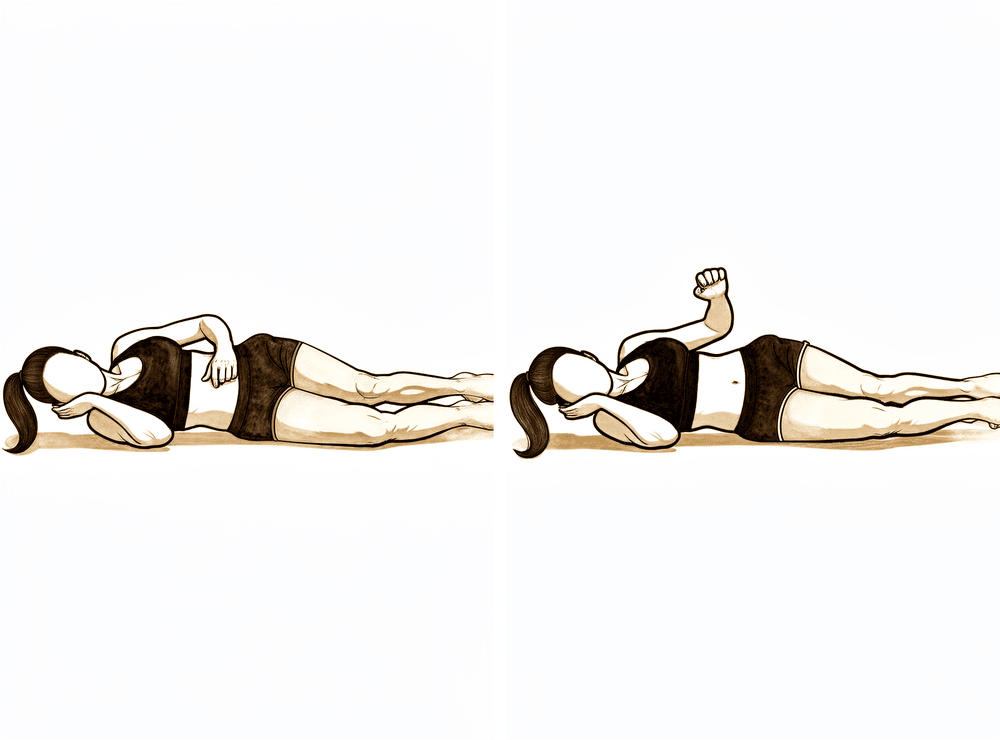
Side-lying external rotation
Lie on your non-operated side with the operated arm on top, elbow bent to 90 degrees and tucked against your body. Keeping the elbow in, rotate the forearm up away from your tummy as far as is comfortable, then lower with control. No added weight — the arm moves under its own power.
As guided by your physiotherapist
Kieran Hirpara 4.0
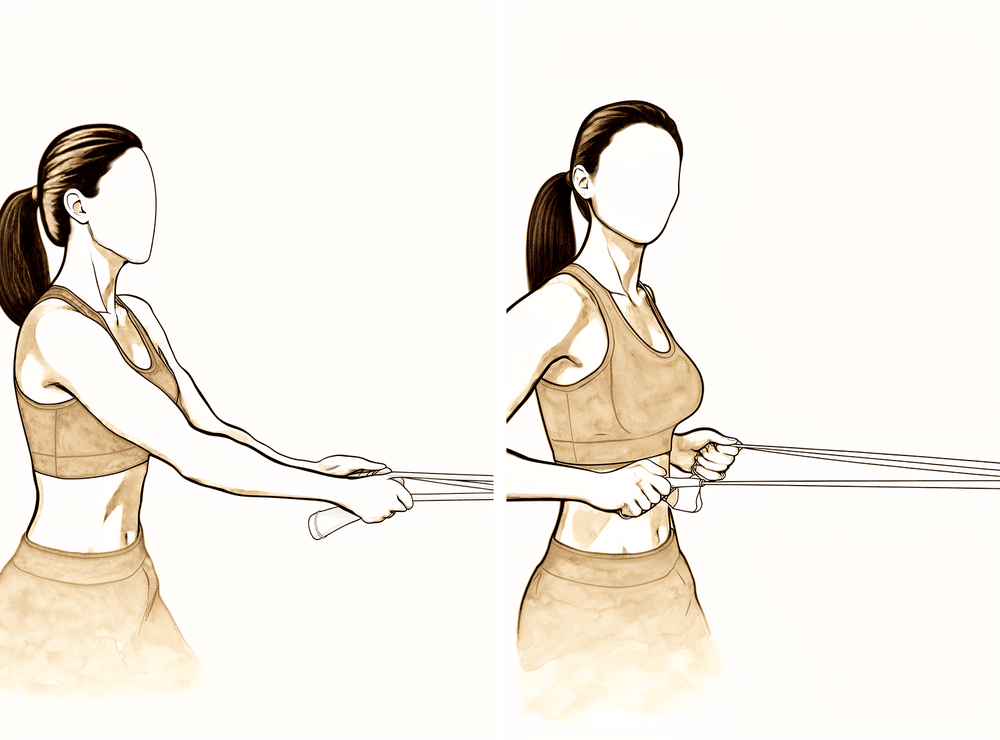
Low row with elastic band
Anchor an elastic band in front of you at waist height. Standing tall, pull the band towards you, drawing the shoulder blade gently down and back, then release with control. Keep the resistance light.
As guided by your physiotherapist
Kieran Hirpara 4.0
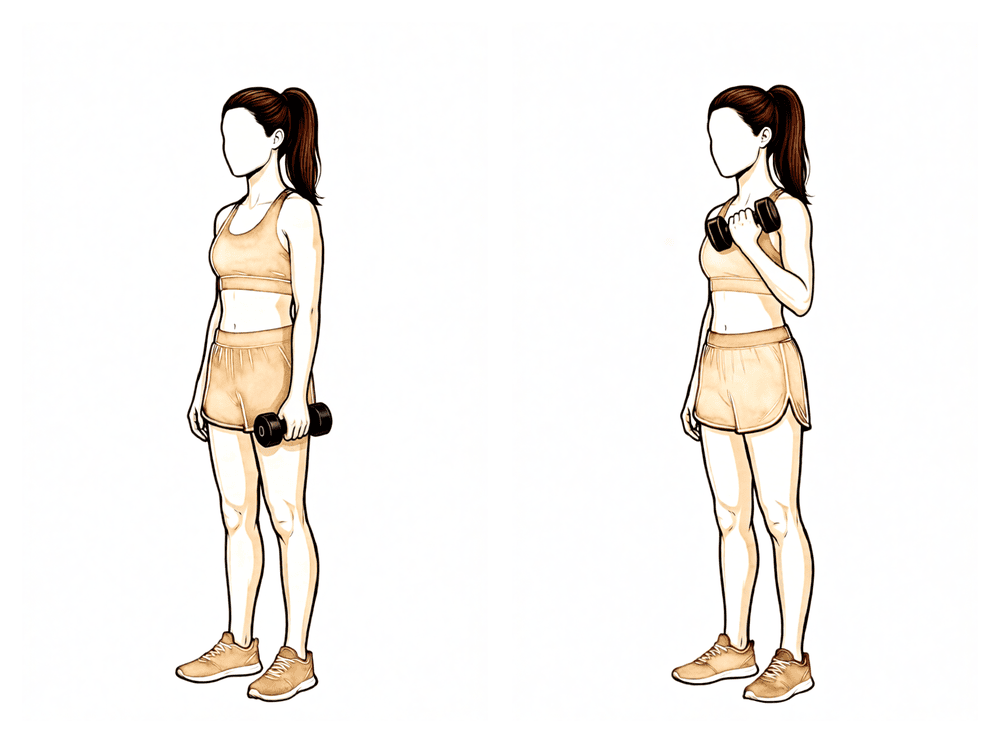
Biceps curls
Holding a light weight with the palm up, bend the elbow to bring the weight towards your shoulder, then lower it slowly. Keep the upper arm still by your side, and keep the weight light — no more than about 1–2 kg in this phase.
As guided by your physiotherapist
Kieran Hirpara 4.0
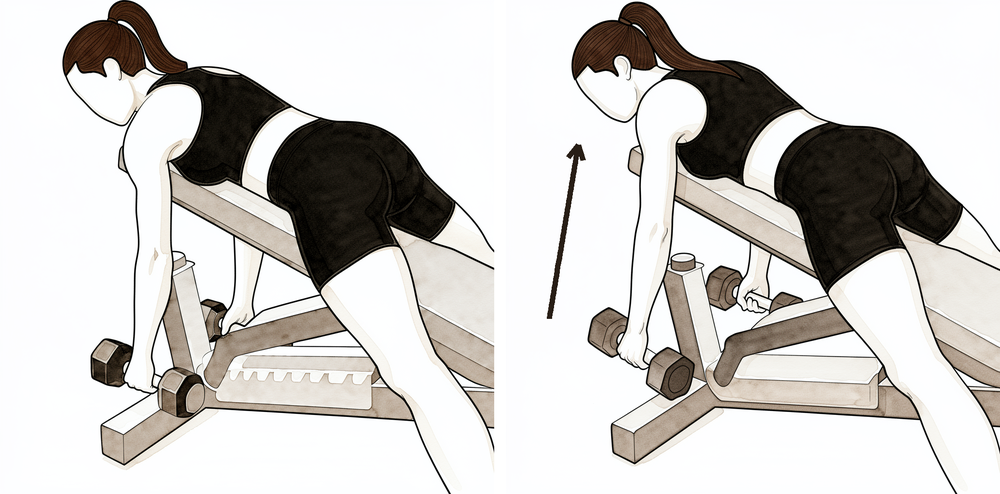
Supported rows
Lean forward with your good arm supported on a table, letting the operated arm hang with a light weight. Draw the shoulder blade back and row the weight up toward your hip, then lower with control. Keep the trunk steady — the movement comes from the shoulder blade and arm, not the back.
As guided by your physiotherapist
Kieran Hirpara 4.0
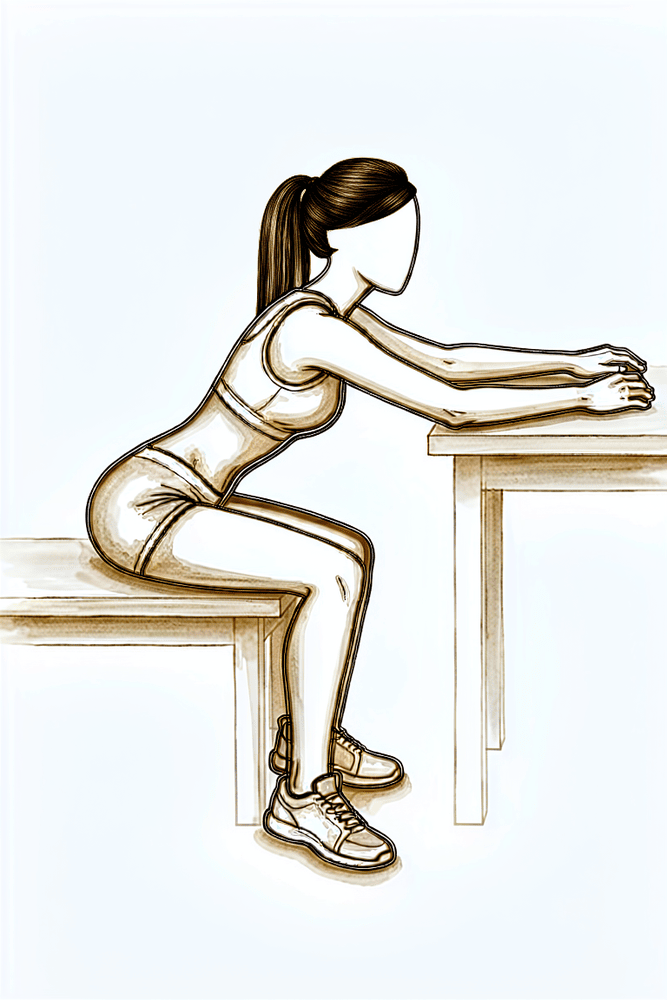
Table slides
Sit at a table with your hand resting on a towel or cloth. Lean forward and slide the hand away from you along the table, letting the arm reach further out in front, then slide it back. The table takes the weight of the arm, so this is a gentle way to regain forward movement.
As guided by your physiotherapist
Kieran Hirpara 4.0
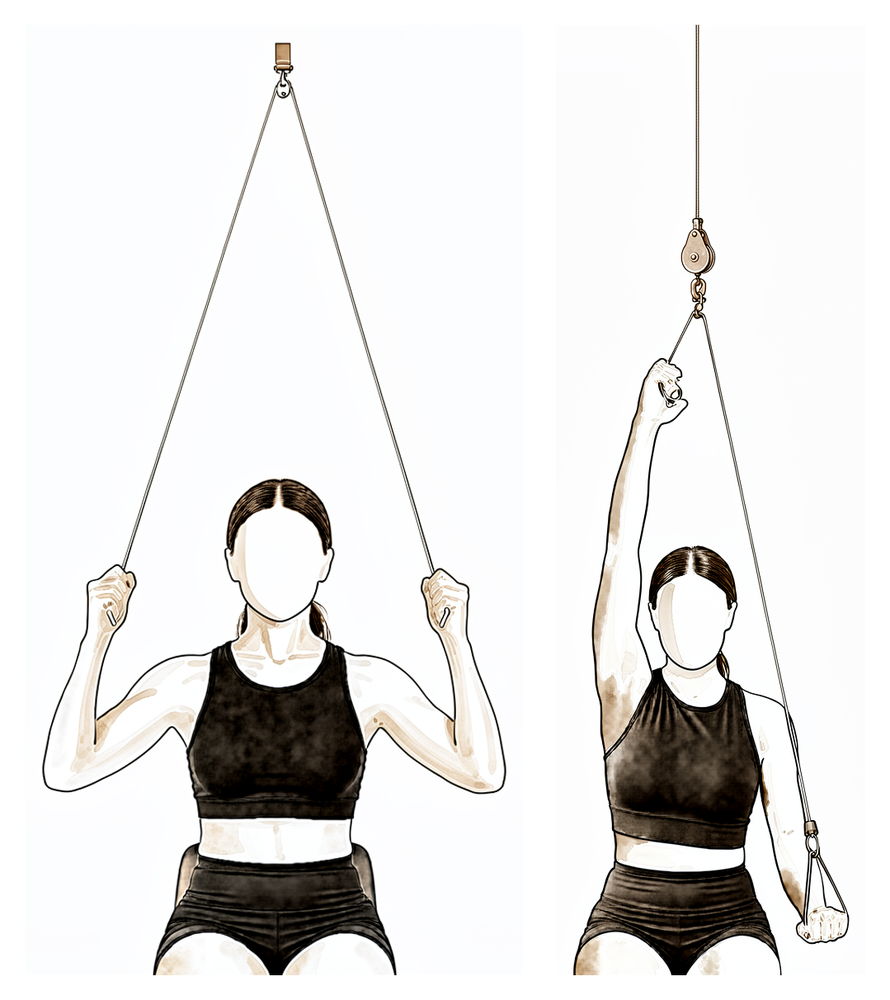
Over-door pulley
Sit under an over-door pulley with a handle in each hand. Pull down with your good arm to raise the operated arm as far as it comfortably goes, then lower it slowly. Let the good arm do the work and stay within a comfortable range.
As guided by your physiotherapist
Kieran Hirpara 4.0
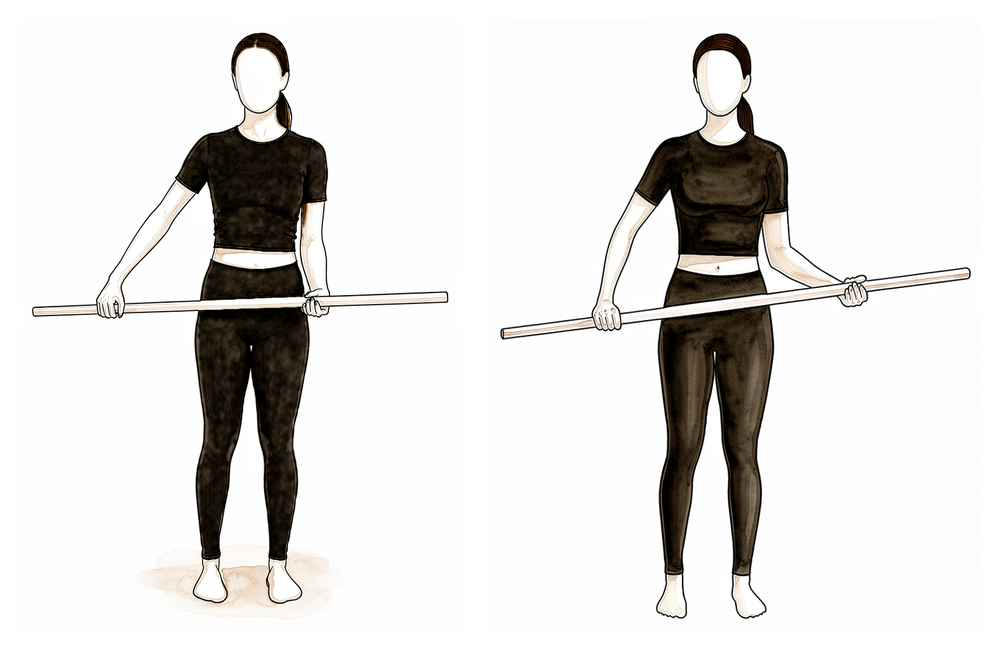
Assisted external rotation with a stick
Lie on your back with the elbow tucked by your side and bent to a right angle. Hold a stick in both hands and use your good arm to turn the operated hand outwards. Once your healing is confirmed, gently work the outward rotation a little further — but stay within the range your surgeon and physiotherapist have set.
As guided by your physiotherapist
Kieran Hirpara 4.0
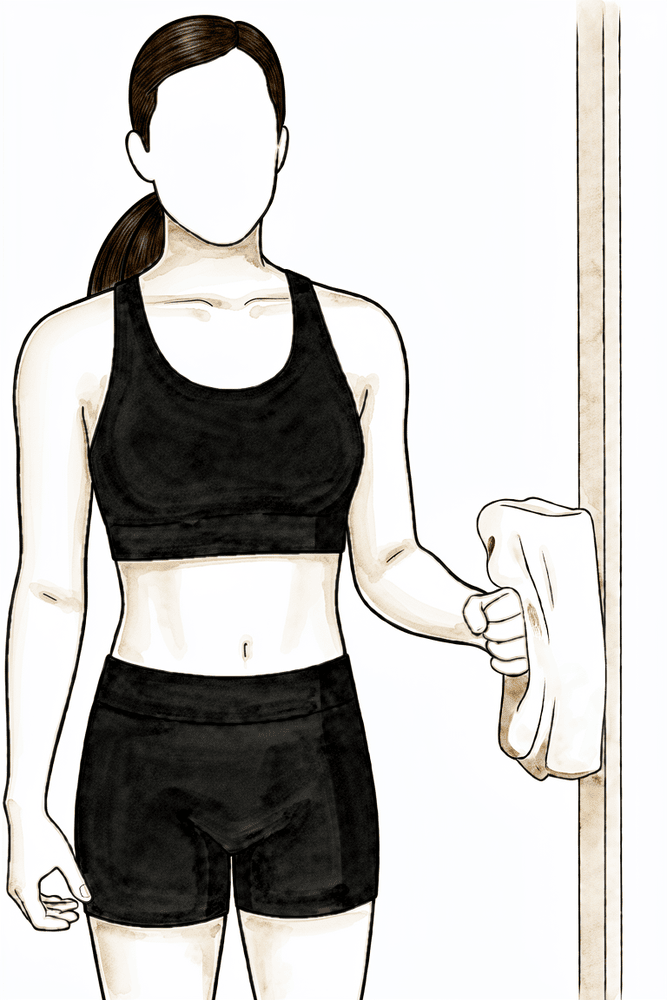
Isometric external rotation
Stand with your elbow tucked at your side and bent to a right angle, the back of your hand against a wall or doorframe. Gently press outwards into it without letting the arm move, hold a few seconds, then relax. This begins to wake up the rotator cuff with no movement — start it only once Dr Hirpara has confirmed your healing.
As guided by your physiotherapist
Kieran Hirpara 4.0
Triceps extensions
Holding a light weight, bend and then straighten the elbow to work the muscle at the back of the upper arm. Keep the upper arm steady and the weight light — no more than about 1–2 kg in this phase.
As guided by your physiotherapist
Kieran Hirpara 4.0
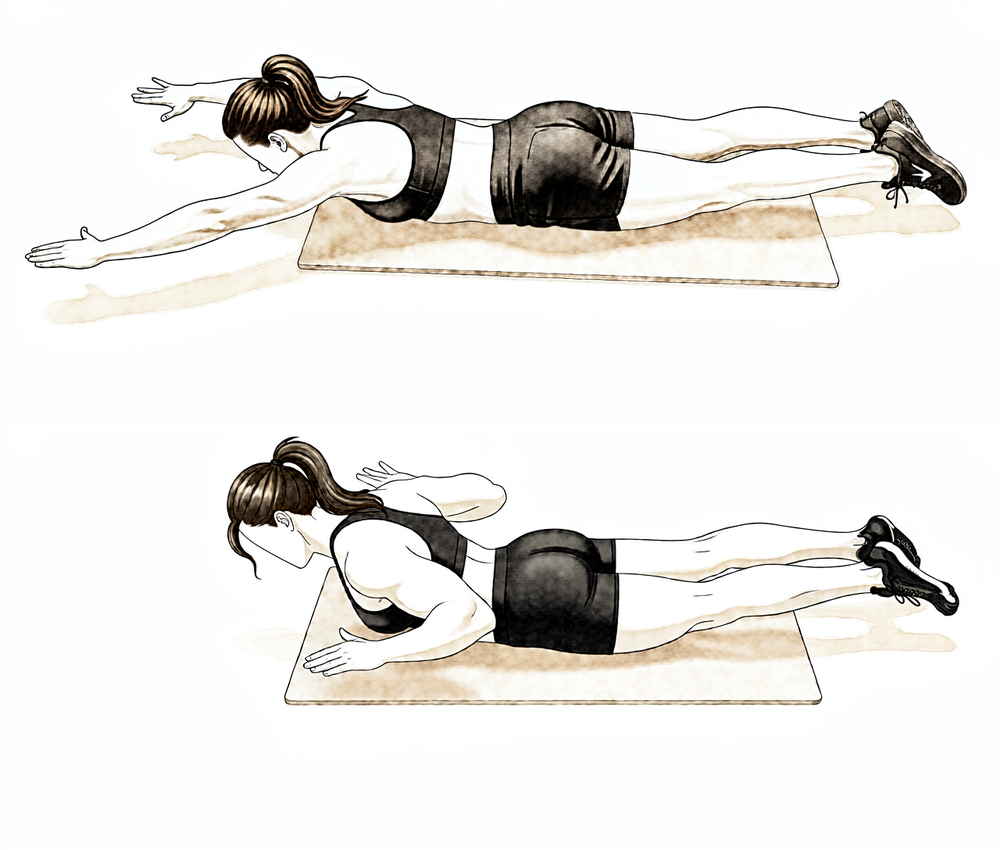
Prone scapular row
Lie face down with your arm hanging over the edge of a bed or bench. Draw the shoulder blade back and lift the arm out to the side a little way, squeezing the shoulder blades together, then lower with control. This strengthens the muscles that steady the shoulder blade.
As guided by your physiotherapist
At your review around six weeks, Dr Hirpara checks your X-rays. If healing is progressing as expected, any remaining sling use stops and you begin moving the arm yourself — first with assistance (using the other arm, a stick or a pulley), then actively. It usually works best to start active lifting of the arm while lying on your back, where gravity is less of an opponent, and progress to sitting and standing as control improves. Gentle muscle-setting (isometric) exercises for the rotator cuff begin in this phase once Dr Hirpara has confirmed healing; exercises against resistance come later. You may return to driving once you are out of the sling, have enough movement and control of the arm to drive safely, and are no longer taking strong painkillers — if in doubt, discuss it at your review.
For your physiotherapist:
Goals
- Restore full passive range of motion
- Progress from active-assisted to active range of motion in all planes
- Re-establish normal scapulohumeral rhythm and minimise compensatory patterns
- Return to normal light daily activities
Management
- Sling fully discarded by the 6-week review at the latest
- Active-assisted range of motion: lawn-chair progression, table / wall slides, pulleys, stick exercises — progressing beyond the Phase I limits as comfort allows
- Active range of motion from about 6–8 weeks: supine flexion progressing to upright elevation; side-lying external rotation and flexion; low rows / low punch
- Submaximal rotator cuff and deltoid isometrics from about 6–8 weeks, with the arm at the side, once healing is confirmed
- Light elbow isotonics (biceps curls, triceps extensions) and scapular strengthening (retraction, prone rows)
- Glenohumeral and scapulothoracic mobilisation as indicated, progressing grades with healing
- Postural correction; continue heat / ice and analgesia around sessions as preferred
Precautions
- No resisted (isotonic) rotator cuff strengthening until union is confirmed — typically not before 8–12 weeks
- No forceful end-range overpressure or aggressive passive stretching
- Lifting limited to about 1–2 kg with the operated arm
- Watch for and correct shoulder hitching and trunk-lean compensation with elevation
Criteria to progress
- Full, or near-full, passive range of motion
- Active elevation with good mechanics, at least below shoulder height
- Isometrics well tolerated without a flare of pain
- Union progressing on X-ray, as confirmed at your review with Dr Hirpara
Phase III — Strengthening (about Months 3 to 4½)¶
Kieran Hirpara 4.0
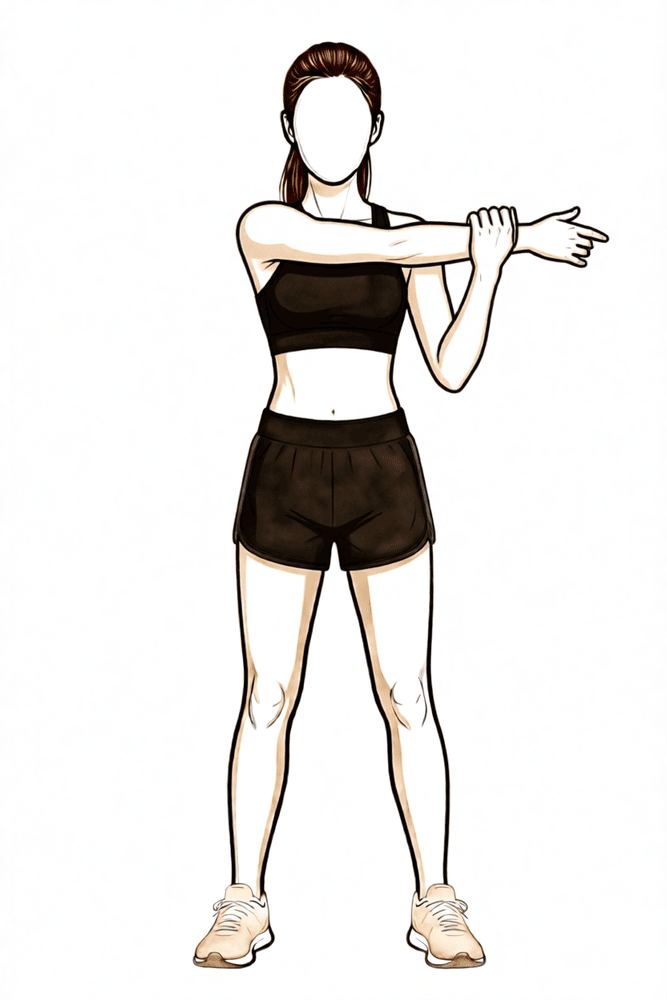
Cross-body stretch
Use your other hand to draw the operated arm across your chest until you feel a stretch at the back of the shoulder. Hold briefly, then release. Stretch to firm discomfort only — never into sharp pain.
As guided by your physiotherapist
Kieran Hirpara 4.0
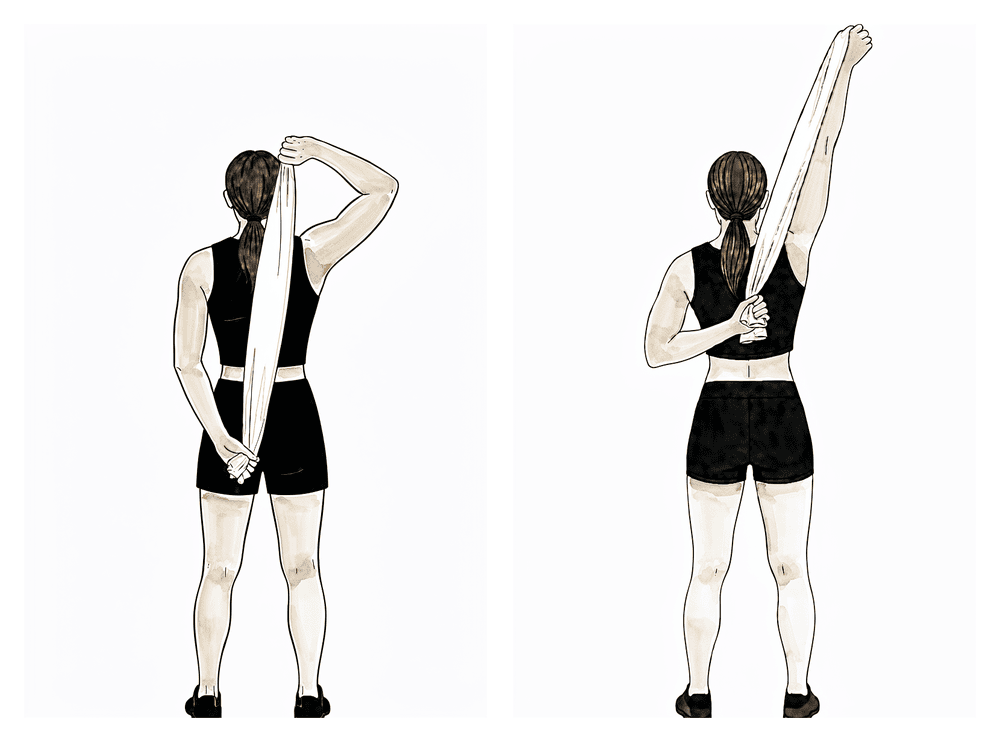
Behind-the-back stretch
Hold a towel behind your back with the good arm above and the operated arm below. Use the upper hand to gently draw the lower hand up your back until you feel a comfortable stretch, hold, then release. Build the range gradually — never force the stretch or push into sharp pain.
As guided by your physiotherapist
Kieran Hirpara 4.0
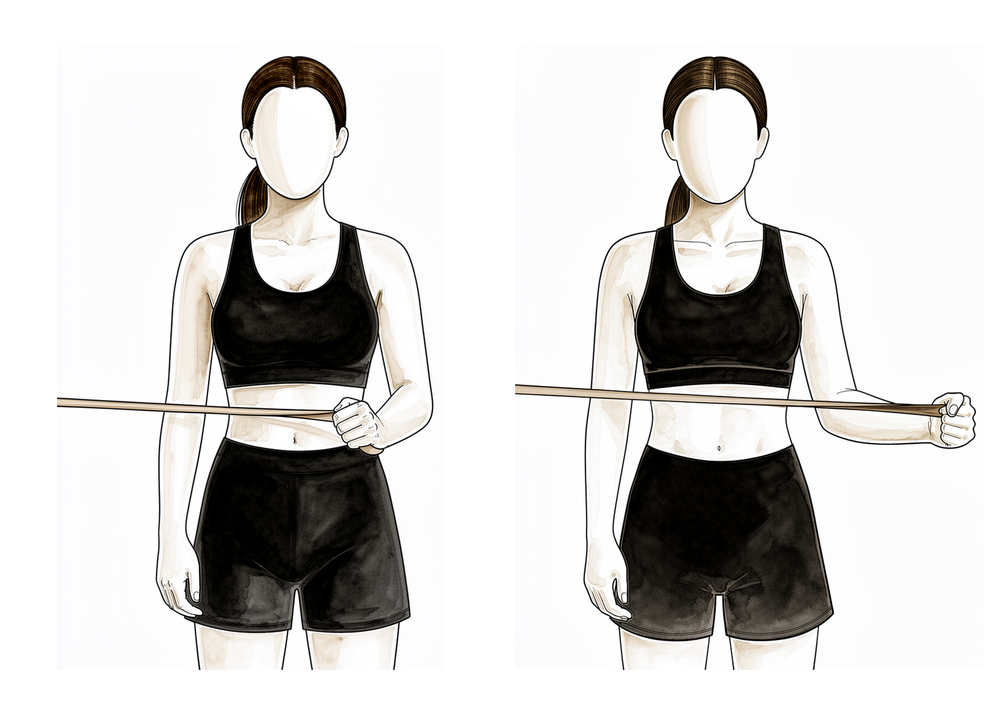
Band external rotation
Stand with your elbow tucked into your side and bent to a right angle, holding an elastic band anchored at waist height. Keeping the elbow at your side, rotate the forearm outwards against the band, then return slowly. This builds the rotator cuff with the arm at the side, the starting point for rotation strengthening.
2 to 3 sets of 8 to 12, low resistance
Kieran Hirpara 4.0
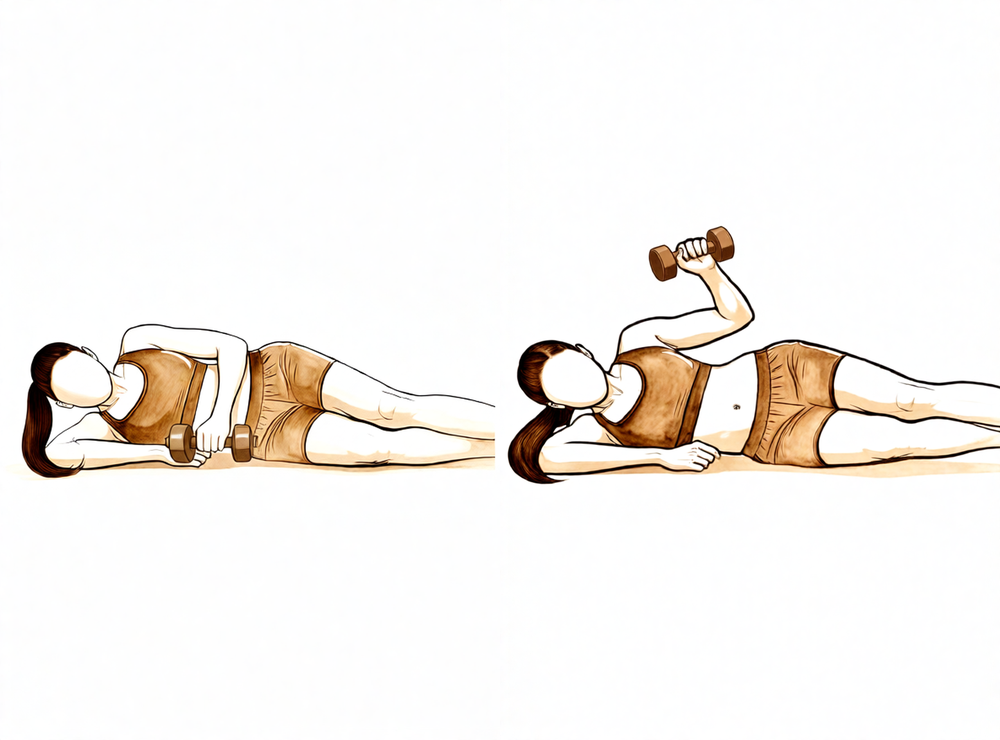
Side-lying external rotation with weight
Lie on your non-operated side with the top elbow bent to a right angle and tucked against your body. Holding a light weight, rotate the forearm up towards the ceiling, then lower slowly. Keep the load light and the repetitions higher as your rotator-cuff strength rebuilds.
2 to 3 sets of 8 to 12, low load
Kieran Hirpara 4.0
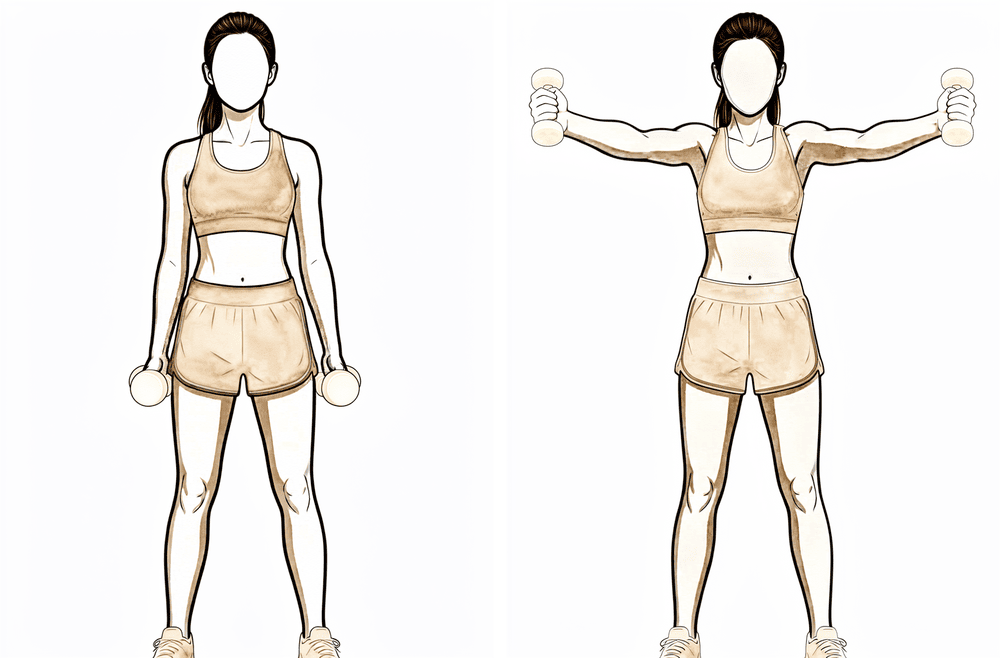
Full-can raise (scaption)
Holding a light weight with your thumb pointing up, raise the arm out to a forward-and-out diagonal — not straight to the side — to about shoulder height, then lower slowly. This works the front of the shoulder and the cuff together. Keep the weight light and stop if it provokes pain that lingers.
2 to 3 sets of 8 to 12, low load
Kieran Hirpara 4.0
Prone row
Lie face down with the operated arm hanging down towards the floor. Draw your elbow up towards the ceiling, squeezing the shoulder blade in towards your spine, then lower slowly. Start with no weight and keep the movement controlled.
As guided by your physiotherapist
Kieran Hirpara 4.0
Doorway chest stretch
Stand in a doorway with your forearms resting on the frame and elbows at about shoulder height. Step one foot through and gently lean forwards until you feel a stretch across the front of your chest, then hold. Keep it gentle and never force it.
Hold ~20–30 seconds, as guided by your physiotherapist
Kieran Hirpara 4.0
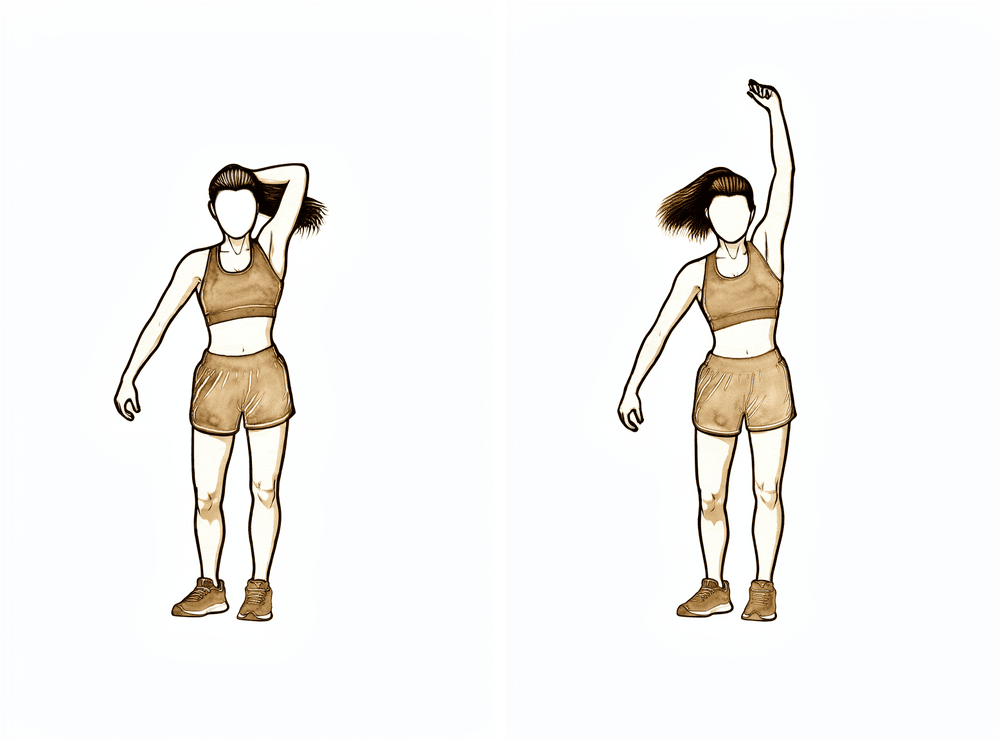
Latissimus (side-of-back) stretch
Reach the operated arm overhead — use your good hand to guide it if needed — and gently lean to the opposite side until you feel a stretch down the side of your back, then hold. Keep it comfortable and within your range.
Hold ~20–30 seconds, as guided by your physiotherapist
With the fracture united and your active movement returning, attention turns to rebuilding strength. Resistance work starts gently — elastic bands and light weights for the rotator cuff, deltoid and shoulder-blade muscles — and progresses gradually. Stretching continues alongside, working towards full movement in all directions, including reaching behind the back. Normal daily activities should be largely back to usual during this phase, and lighter recreational activities typically resume, as guided by your physiotherapist.
For your physiotherapist:
Goals
- Full active range of motion in all planes with normal mechanics
- Graduated restoration of rotator cuff, deltoid and scapular strength and endurance
Management
- Progress from isometrics to elastic-band and then light free-weight strengthening (about 0.5–2 kg) for the cuff, deltoid and scapular stabilisers — low load, higher repetitions (for example 2–3 sets of 8–12), resistance sessions about 3 times per week to avoid overload
- Rotation strengthening initially with the arm at the side, below shoulder height
- Emphasise anterior deltoid and the trapezius–serratus anterior force couple for a stable scapular base
- Flexibility program for terminal range in all planes: posterior capsule (cross-body) stretch, behind-the-back internal rotation, anterior chest wall / pectoralis minor stretches, doorway stretch
- Begin internal rotation behind the back and grade III–IV mobilisations as range allows
- Upper-body ergometer with low resistance; general aerobic conditioning
Precautions
- Strengthening stays within the comfortable range and should not provoke pain that lingers
- No lifting greater than about 4–5 kg with the operated arm during this phase
- Avoid excessive weight-bearing through the arm (push-ups and similar come later)
Criteria to progress
- Full active range of motion with no compensatory strategies
- Strengthening program tolerated without flare-up of pain or loss of range
Phase IV — Return to full activity (from about 4½–6 months)¶
The final phase is a graduated return to heavier lifting, manual work, overhead tasks and sport. Strength work advances to heavier resistance and compound movements, and — where it is relevant to your work or sport — to faster, more dynamic exercise. Most people are back to their usual activities by around six months, though strength and confidence typically keep improving for up to a year. The right finish line depends on what you need the arm to do, so the return to heavy manual work or contact and overhead sport is agreed with Dr Hirpara and your physiotherapist rather than set by the calendar.
For your physiotherapist:
Goals
- Return to full work, recreational and sporting activity
- Strength of the operated arm approaching that of the other side
Management
- Progressive resistance through bands, free weights and gym-based compound movements
- Push-up progression (wall → bench → knees → full) and closed-chain stability work as tolerated
- From about 4½ months: eccentric loading, plyometrics (weighted-ball work), proprioceptive and rhythmic-stabilisation drills where relevant
- Resisted rotation at 90° of elevation, and interval sport-specific or vocation-specific programs as appropriate
Precautions
- Progression remains symptom-guided — if pain or loss of range recurs, ease back and restore comfortable movement first
Criteria to discharge
- Strength of the operated arm at least about 80% of the other side where measured
- No pain with progressive strengthening
- Independent with a maintenance home program
After your protocol¶
The phases above are adapted from published rehabilitation protocols for proximal humerus fracture fixation — Massachusetts General Brigham Sports Medicine, Twin Cities Orthopedics, the UConn Musculoskeletal Institute, NYU Langone Orthopedic Center and South Bend Orthopaedics — together with a systematic review of rehabilitation after proximal humerus fracture. Published protocols for this operation vary more than for most shoulder surgery, because the right pace depends on how the individual fracture was fixed and how it heals; your progression through the phases is therefore directed by Dr Hirpara at your reviews and adjusted by your physiotherapist between them. This page works alongside the practice's general recovery advice — see managing post-operative pain and wound care. For the operation itself, see proximal humerus fixation.
If you would like to read the evidence behind this protocol — the research on early versus delayed movement after plate fixation, the surgery-versus-sling debate, and the complications the staged progression is designed to avoid — a fully referenced evidence summary is available as a PDF alongside this page.
Evidence & references
Proximal Humerus Fracture Fixation (Locking-Plate ORIF) — Post-operative Rehabilitation: Evidence¶
Topic scope: Post-operative rehabilitation after open reduction and internal fixation (ORIF) of a proximal humerus fracture with a locking (angular-stable) plate and screws. This page covers the evidence behind the phased rehabilitation program — early protected/passive motion, deferred active and resisted motion, and graded strengthening — and the surgical-outcome facts that shape it. It does not cover the separate pathways of non-operative fracture management, intramedullary nailing, hemiarthroplasty or reverse total shoulder arthroplasty, although the operative-versus-non-operative debate is summarised because it frames who is offered this operation at all.
Defining principle of the rehab here (mobilise early, protect the tuberosities): A locking plate is an angular-stable construct — the screws lock into the plate, so the fixation holds even in osteoporotic bone without relying on bone-to-screw friction. Because that stability is present from day one, this protocol now permits early active (and active-assisted) shoulder elevation in a pain-free range for stable fixation, consistent with the early-active-motion RCT evidence (Loew 2025), rather than holding the shoulder passive-only for six weeks. The element still keyed to biological healing is rotation and rotator-cuff loading: where the tuberosity fragments to which the rotator cuff attaches are part of the fracture, active/resisted rotation and cuff work are held back until those fragments unite, whereas where the tuberosities are uninvolved or solidly fixed the surgeon may clear cuff loading sooner. The brake is therefore biological, not mechanical — the plate is strong immediately — and it is now selective (rotation/cuff), not a blanket movement ban. Progression of cuff loading remains governed by fracture stability and radiographic healing, not the calendar. This places the protocol close to the early-active-movement end of the spectrum while still being more tuberosity-aware than a pure debridement/decompression, and far less tuberosity-dependent than a fracture arthroplasty, where healing of the tuberosities to the prosthesis dictates a slower, stricter cuff-loading timetable.
The operation¶
A proximal humerus fracture is a break of the upper end of the arm bone, near the shoulder. In ORIF the fragments are realigned (reduced) and held with a pre-contoured locking plate on the outer surface of the bone, fixed with multiple locking screws into the humeral head. Where the tuberosities (the bony knobs carrying the rotator-cuff attachments) are part of the fracture, they are reduced and secured to the plate, often reinforced with heavy sutures through the cuff. The plate provides immediate mechanical stability; the rehabilitation then protects the biological healing of the fracture and the tuberosity fragments.
Evidence by theme¶
1. Modern locking plates permit early active motion — supported by RCT evidence and adopted here for stable fixation¶
The historical "restrictive" protocol kept the arm immobilised with no active movement for ~6 weeks, with passive limits of flexion to ~90°, external rotation to ~20° and internal rotation to the belly. The rationale for early motion is to prevent the shoulder stiffening (adhesive capsulitis is a recognised complication of these fractures) while still protecting the bone. Because an angular-stable locking plate is mechanically strong from day one, early active elevation can be permitted for stable fixation; the element kept keyed to biological healing is rotation and rotator-cuff loading, because that is what pulls on the tuberosity fragments.
The more aggressive question — can patients move actively from the start? — has now been tested. A prospective randomised controlled trial (Loew et al., J Orthop, 2025) compared a conventional 4-week sling-immobilisation group against an early functional group with no movement or force restrictions after locking-plate ORIF (both groups avoided heavy lifting and impact for 3 months). At 24 months there was no significant difference in DASH or Constant score: Constant score averaged 81.3 (conventional) vs 78.4 (early functional), with relative Constant score 89.8% of the uninjured side in both groups — i.e. early active motion was non-inferior. Moderate (single RCT). This is consistent with the broader signal that early intensive mobilisation yields similar outcomes to conventional later mobilisation after operative treatment. In line with this evidence, Dr Hirpara's protocol now permits early active elevation in a pain-free range for stable fixation; the literature still has no consensus on the optimal regimen, so the one element kept deliberately cautious and keyed to radiographic healing is active/resisted rotation and rotator-cuff loading, because that is the movement that stresses the healing tuberosity fragments.
2. Post-operative protocols are highly heterogeneous, but converge on short immobilisation and early passive ROM¶
The best summary of practice is a systematic review of 45 cohorts (40 articles, 3,507 patients, 3,519 fractures) (Budharaju et al., Shoulder Elbow, 2024). Across studies:
- Sling immobilisation averaged 3.1 weeks (most commonly 3 weeks; range 0–6).
- Passive ROM began at ~0.9 weeks on average (most commonly at 2 days).
- Active ROM began at ~2.5 weeks on average (most commonly at 3 weeks).
- Strengthening began at ~5.5 weeks on average (most commonly at 6 weeks).
The authors emphasised substantial variability regardless of management, concluded that this heterogeneity limits cross-study comparison, and noted that early mobilisation may produce superior function — supporting consideration of shorter immobilisation. The synthesis page's "~3 weeks in the sling, then wean" reflects this averaged convention, not a trial-proven optimum. Moderate for the descriptive pattern; weak/consensus for any specific timetable.
3. Progression is governed by fracture stability and healing, not the calendar — because of the tuberosities and biological complications¶
The locking plate is strong immediately; what limits the rehab is the bone. Two facts anchor the "wait-for-healing" rule:
- Tuberosity / cuff loading. When the tuberosities are part of the fracture, loading the rotator cuff (forced/resisted external rotation and resisted cuff work) too early risks displacing fragments before they unite. This is the explicit reason the early phases keep rotation cautious and defer cuff loading until healing, even though early active elevation in a pain-free range is permitted; where the tuberosities are uninvolved or solidly fixed, the surgeon may clear cuff loading sooner.
- The major complications of locking-plate ORIF are largely biological and mechanical, and several are loading- and reduction-sensitive. A systematic review (Thanasas / Brorson-class series) reports the commonest complications as intra-articular screw perforation (~9–12%), varus collapse (~6.8%), loss of reduction, avascular necrosis of the humeral head (~4.6%, reported range 0–15%), subacromial impingement (~5%), adhesive capsulitis (~4%), nonunion (~1.5%) and deep infection (~1.4%). Screw perforation and avascular necrosis frequently coincide, because a head that collapses or undergoes AVN lets fixed-length locked screws migrate into the joint. Moderate (pooled observational series).
This complication profile is why progression waits on radiographs: premature loading risks tipping a borderline reduction into varus collapse or screw cut-out. Some surgeons even advocate early planned plate removal to avoid secondary screw penetration once the head shows AVN/collapse (Dimitriou et al., J Orthop, 2019) — a salvage strategy, not part of routine rehab, but it illustrates how mechanical and biological failure interact.
4. Who is offered ORIF at all — the operative-versus-non-operative debate (PROFHER and after)¶
The single most influential trial is PROFHER (Rangan et al., JAMA, 2015; 250 patients, 32 UK centres, displaced fractures involving the surgical neck): surgery showed no important difference in Oxford Shoulder Score versus sling-based non-operative care over 2 years, and was more expensive. The 5-year follow-up (Handoll/Keding et al., Bone Joint J, 2017) confirmed no significant difference in shoulder function or quality of life persisting to 5 years. A smaller RCT in displaced 3-part fractures in the elderly (Fjalestad et al., J Shoulder Elbow Surg, 2012) similarly found no functional advantage to internal fixation over non-operative care in that group, and a systematic review and meta-analysis (Beks et al., J Shoulder Elbow Surg, 2018) found no clear superiority of operative treatment across observational and randomised data combined. Strong (multiple RCTs + SR-MA).
The clinical upshot — and the reason this matters to a rehab page — is that ORIF is selectively indicated, typically in younger patients, in fractures where reduction and stable fixation are achievable and worthwhile, and where the alternative (non-operative care or arthroplasty) is judged less favourable. The decision is individualised; "difficulty in decision-making" for displaced fractures is itself documented as affecting outcomes (Okike et al., J Shoulder Elbow Surg, 2018). Patients should understand that being offered ORIF is a considered judgement, not an automatic consequence of the fracture.
5. Adjacent rehabilitation evidence (non-operative immobilisation duration)¶
Although it concerns non-operatively treated fractures, a relevant randomised controlled trial (Tanji et al., J Bone Joint Surg Am, 2021) compared 1 versus 3 weeks of immobilisation and supports the broad theme that earlier movement is at least as good as longer immobilisation for many proximal humerus fractures. It does not directly govern the post-ORIF protocol but reinforces the same direction-of-travel away from prolonged slings. Moderate (RCT, non-operative population).
Phased post-operative timeline (consistent with the synthesis page)¶
| Phase | Window | Sling | Shoulder motion | Strengthening | Governing rule |
|---|---|---|---|---|---|
| I — Protection & early passive motion | Weeks 0–6 | Full-time ~3 weeks, then weaned; off for exercises/hygiene; not in bed | Early active-assisted/active elevation permitted in a pain-free range from the outset (supine-start → upright); passive as needed; pendulums; elbow/wrist/hand active. ER kept to a gentle ~30–40° default; rotation cautious — defer active/resisted cuff work until tuberosities heal (surgeon-guided) | None at the shoulder (deltoid/periscapular isometrics as comfort allows) | Protect fixation + tuberosities; settle pain/swelling |
| II — Regaining active movement | Weeks 6–12 | Discarded by the 6-week review at the latest | Active-assisted → active in all planes (supine-start elevation); submaximal cuff/deltoid isometrics once healing confirmed | Light elbow/scapular work; no resisted cuff work until union (typically not before 8–12 weeks) | Radiographic healing at the ~6-week review gates active motion |
| III — Strengthening | ~Months 3–4½ | Off | Full active ROM in all planes, including behind-the-back | Graded bands → light free weights (~0.5–2 kg) for cuff, deltoid, scapula | Union confirmed; symptom-guided load progression |
| IV — Return to full activity | ~4½–6 months | Off | Full, with dynamic/overhead drills as relevant | Heavier resistance, compound + sport/work-specific | Return-to-task agreed with surgeon/physio, not the calendar |
The phase boundaries are individualised at Dr Hirpara's reviews on the basis of X-ray healing — this is the operative consequence of the "stability- and healing-governed, not calendar-governed" principle.
Key controversies / evidence quality¶
-
Early active versus delayed (protected) mobilisation after ORIF. A single RCT (Loew 2025) found unrestricted early active motion non-inferior to 4-week immobilisation at 24 months, and the broader literature leans toward shorter immobilisation. The protocol here aligns with that early-active-motion evidence: early active and active-assisted elevation in a pain-free range is permitted for stable fixation, rather than holding the shoulder passive-only for six weeks. Because there is still no consensus and no large confirmatory trial (protocols remain heterogeneous — Budharaju 2024), the protocol keeps one deliberate, evidence-aware caution: active/resisted rotation and cuff loading is keyed to radiographic tuberosity healing rather than released wholesale on day one. Moderate evidence, unsettled.
-
Operative versus non-operative treatment of displaced fractures. PROFHER (2015) and its 5-year follow-up (2017), plus an elderly-3-part RCT (Fjalestad 2012) and a meta-analysis (Beks 2018), found no clear functional benefit of surgery on average — which is why ORIF is selectively, not routinely, offered. The trials enrolled broad/older populations; the subgroup most likely to benefit from fixation (younger patients, good bone, reconstructable head-preserving fractures) is exactly where this operation is concentrated. Strong evidence overall; subgroup benefit remains debated.
-
The post-operative rehab protocol itself is consensus/expert. No high-level RCT defines the optimal phase structure, ROM limits or strengthening onset after ORIF. The timings here are drawn from published surgeon protocols and the systematic-review averages, individualised at review. Weak/consensus.
Evidence-strength flags (summary)¶
- STRONG (RCT / SR-MA): operative versus non-operative equivalence on average for displaced fractures (PROFHER 2-yr JAMA 2015 + 5-yr Bone Joint J 2017; Fjalestad 2012 RCT; Beks 2018 SR-MA).
- MODERATE (single RCT / pooled series): early active motion non-inferior to immobilisation after ORIF at 24 months (Loew 2025 RCT); 1-vs-3-week immobilisation non-operatively (Tanji 2021 RCT); locking-plate complication profile — screw perforation, varus collapse, AVN, etc. (pooled observational series); descriptive practice pattern of short sling + early passive ROM (Budharaju 2024 SR of 45 cohorts).
- WEAK / CONSENSUS: the specific phased rehabilitation timetable after ORIF (no defining rehab RCT; published surgeon protocols + systematic-review averages; progression individualised by radiographic healing).
Citations¶
RAG corpus (180,000+ Orthopaedic articles) — real DOIs¶
- Five-year follow-up results of the PROFHER trial comparing operative and non-operative treatment of adults with a displaced fracture of the proximal humerus. Bone Joint J. 2017. DOI: 10.1302/0301-620x.99b3.bjj-2016-1028
- Operative versus nonoperative treatment of proximal humeral fractures: a systematic review, meta-analysis, and comparison of observational studies and randomized controlled trials. J Shoulder Elbow Surg. 2018. DOI: 10.1016/j.jse.2018.03.009
- Internal fixation versus nonoperative treatment of displaced 3-part proximal humeral fractures in elderly patients: a randomized controlled trial. J Shoulder Elbow Surg. 2012. DOI: 10.1016/j.jse.2010.12.018
- One Versus 3-Week Immobilization Period for Nonoperatively Treated Proximal Humeral Fractures: a randomized controlled trial. J Bone Joint Surg Am. 2021. DOI: 10.2106/jbjs.20.02137
- Contemporary Management of Proximal Humeral Fractures. J Am Acad Orthop Surg. 2024. DOI: 10.5435/jaaos-d-24-01073
- The Use of Precontoured Humeral Locking Plates in the Management of Displaced Proximal Humerus Fracture. J Am Acad Orthop Surg. 2009. DOI: 10.5435/00124635-200909000-00005
- Use of locking plates in the treatment of proximal humerus fractures. J Shoulder Elbow Surg. 2010. DOI: 10.1016/j.jse.2010.01.001
- Functional results and unfavorable events after treatment of proximal humerus fractures using a new locking plate system. BMC Musculoskelet Disord. 2023. DOI: 10.1186/s12891-023-06176-5
- Fracture site augmentation with calcium phosphate cement reduces screw penetration after open reduction–internal fixation of proximal humeral fractures. J Shoulder Elbow Surg. 2012. DOI: 10.1016/j.jse.2011.09.017
- Difficulty in decision making in the treatment of displaced proximal humerus fractures: the effect of uncertainty on surgical outcomes. J Shoulder Elbow Surg. 2018. DOI: 10.1016/j.jse.2017.09.033
Literature (URLs)¶
- Loew M, et al. Postoperative treatment of proximal humerus fractures with an early active motion protocol: a prospective randomized controlled trial. J Orthop. 2025. https://www.sciencedirect.com/science/article/pii/S1058274625001867 (Constant 81.3 conventional vs 78.4 early-functional at 24 months; early active motion non-inferior)
- Budharaju A, Hones KM, Hao KA, et al. Rehabilitation protocols in proximal humerus fracture management: a systematic review. Shoulder Elbow. 2024;16(4):449–458. https://pmc.ncbi.nlm.nih.gov/articles/PMC11437559/ (45 cohorts; sling 3.1 wk, passive 0.9 wk, active 2.5 wk, strengthening 5.5 wk; early mobilisation may improve function)
- Rangan A, et al. (PROFHER). Surgical vs nonsurgical treatment of adults with displaced fractures of the proximal humerus: the PROFHER randomized clinical trial. JAMA. 2015;313(10):1037–1047. https://pubmed.ncbi.nlm.nih.gov/25756440/ (250 patients; no important difference in Oxford Shoulder Score at 2 years)
- Complications associated with locking plate of proximal humerus fractures (systematic review of complication rates). PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC5858203/ (screw perforation ~9–12%, varus collapse ~6.8%, AVN ~4.6%)
- Avascular necrosis and posttraumatic arthritis after proximal humerus fracture internal fixation: evaluation and management. PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC9889581/ (AVN reported range 0–15%)
- Late screw-related complications in locking plating of proximal humerus fractures: a systematic review. Injury. https://www.sciencedirect.com/science/article/abs/pii/S0020138319306989
- Dimitriou D, et al. Early locking plate removal following ORIF of proximal humeral fractures could prevent secondary implant-related complications. J Orthop. 2019;17:106–109. https://pmc.ncbi.nlm.nih.gov/articles/PMC6919395/
Published rehabilitation protocols (patient-guidance — basis for the phase structure)¶
- Massachusetts General Brigham Sports Medicine. Rehabilitation Protocol for Proximal Humeral Fracture Open Reduction Internal Fixation (ORIF). https://www.massgeneral.org/assets/MGH/pdf/orthopaedics/sports-medicine/physical-therapy/rehabilitation-protocol-for-proximal-humeral-fracture-with-ORIF.pdf
- LaPrade CM. Post-Surgical Physical Therapy Protocol: Proximal Humerus Fracture ORIF. Twin Cities Orthopedics. https://tcomn.com/wp-content/uploads/2024/08/CML_Proximal-Humerus-ORIF-PT_10-2024.pdf
- Coyner KJ. ORIF Proximal Humerus Fractures Protocol. UConn Musculoskeletal Institute. https://www.drcoyner.com/pdf/orif-proximal-humerus-fractures-protocol.pdf
- Jazrawi LM. Rehabilitation Protocol: Proximal Humerus Open Reduction & Internal Fixation (ORIF). NYU Langone Orthopedic Center. https://www.newyorkortho.com/pdf/proximal-humerus-fracture-orif-post-op-instructions-and-rehab.pdf
- South Bend Orthopaedics. ORIF Proximal Humerus Fracture Rehab Protocol. https://www.sbortho.com/wp-content/uploads/2023/09/br-pt-fracture-orif-proximal-humerus.pdf