Capsular Release PDF Evidence¶
Rehabilitation after arthroscopic capsular release for frozen shoulder — early in-hospital program and the outpatient phases that keep the range won at surgery.
This protocol covers the rehabilitation after an arthroscopic capsular release with Dr Kieran Hirpara at Mater Private Hospital Rockhampton, both what happens in hospital and over the weeks and months afterwards. Bring this page or its PDF to your first physiotherapy visit so your rehabilitation stays coordinated. Your rehabilitation is progressed individually by your physiotherapist through the phases below, depending on how your shoulder is moving.
If you have any concerns about your wound after surgery, get in touch with the rooms. It is often helpful to take a photo of the wound and email it for review.
What to expect¶
Capsular release is an operation for a stiff shoulder (frozen shoulder), and that changes everything about how you rehabilitate. Most shoulder operations repair something, such as a tendon or a torn ligament, and the early job is to protect that repair, so you wear a sling and keep movement within limits. This operation is the opposite. Nothing has been stitched back together that needs protecting. The surgeon has released the tight, scarred lining of the joint and moved the shoulder through a full range while you were asleep, so the result of the operation is the movement. From the moment you wake up, the job of rehabilitation is to keep that movement before the shoulder tries to stiffen up again.
That means there is no protected period and no holding back. You start moving the shoulder straight away, both moving it yourself and using your other arm to push it, and you keep pushing the range, in every direction, several times a day.
Your exercises use three kinds of movement, and your team will mark which apply to you:
- Passive movement means the shoulder stays completely relaxed while your other arm, a stick or a pulley does all the work.
- Active-assisted movement means you move the arm yourself with some help from the other arm or an object.
- Active movement means you move the arm under its own power, without help.
Why there is no sling¶
After a capsular release there is no sling to protect a repair, and keeping the shoulder still is the one thing that works against you. Left to rest, the released shoulder simply tightens up again. Re-stiffening is the main reason this operation can disappoint, and it is largely preventable by moving early and often.
So unlike a repair, you do not sleep in a sling, you do not keep the arm still, and there is no movement that is off-limits. You are encouraged to use the arm freely and to push your range in every direction, including rotating the arm outwards, right from day one. A simple sling is offered only for short-term comfort and to stop the arm being knocked when you are out and about; leave it off as much as you can and do not let it tempt you into keeping the shoulder still.
Key points¶
- Keep moving. Use the arm for normal everyday tasks such as washing, dressing and eating, from the start. Movement keeps the range you gained at surgery.
- Push the range, in every direction. Stretch to the point of firm discomfort, not severe pain, and take the shoulder to its limit in every plane, including rotating the arm outwards. There is no "do not go past here" precaution after this operation.
- Stretch little and often. A short home stretching program done several times a day beats one long session. Re-stiffening happens between sessions, so frequency matters.
- Control the pain so you can move. Take your pain relief before your exercises and before your physiotherapy appointments. Good pain control is what makes the stretching possible. Many people find heat before stretching and ice afterwards helpful.
- Go to physiotherapy often. Aim for at least twice a week for the first six weeks. Bring this page to your first visit.
A steroid is often injected into the joint at the time of the operation to calm the inflammation and reduce the tendency to re-stiffen.
In hospital — your first exercises¶
Kieran Hirpara 4.0
Wrist movement
Keep your hand moving by bending your wrist forwards, backwards and side to side.
10 times, 3 times per day
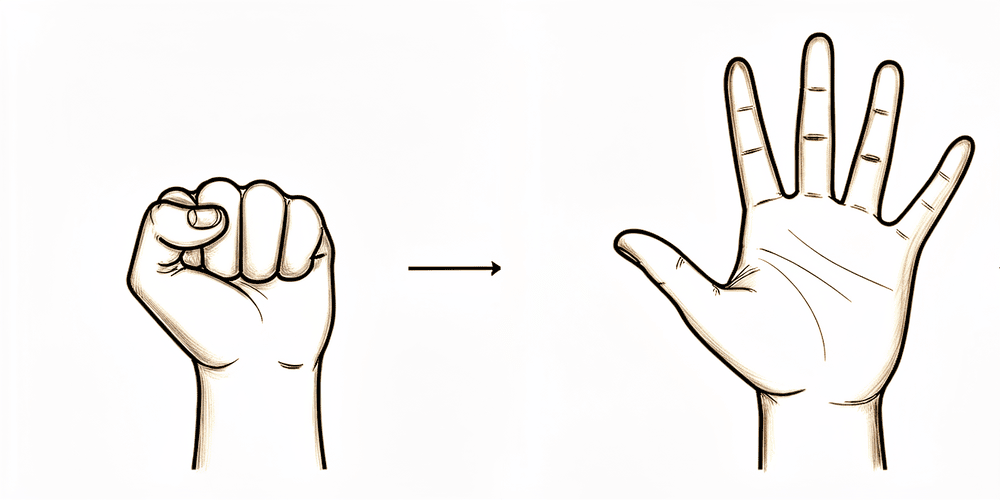
Kieran Hirpara 4.0
Open and close hand
Keep your hand and fingers moving by opening and closing them, or by squeezing a soft ball.
10 times, 3 times per day
Kieran Hirpara 4.0
Elbow bends
Bend and straighten your elbow.
10 times, 3 times per day
Kieran Hirpara 4.0
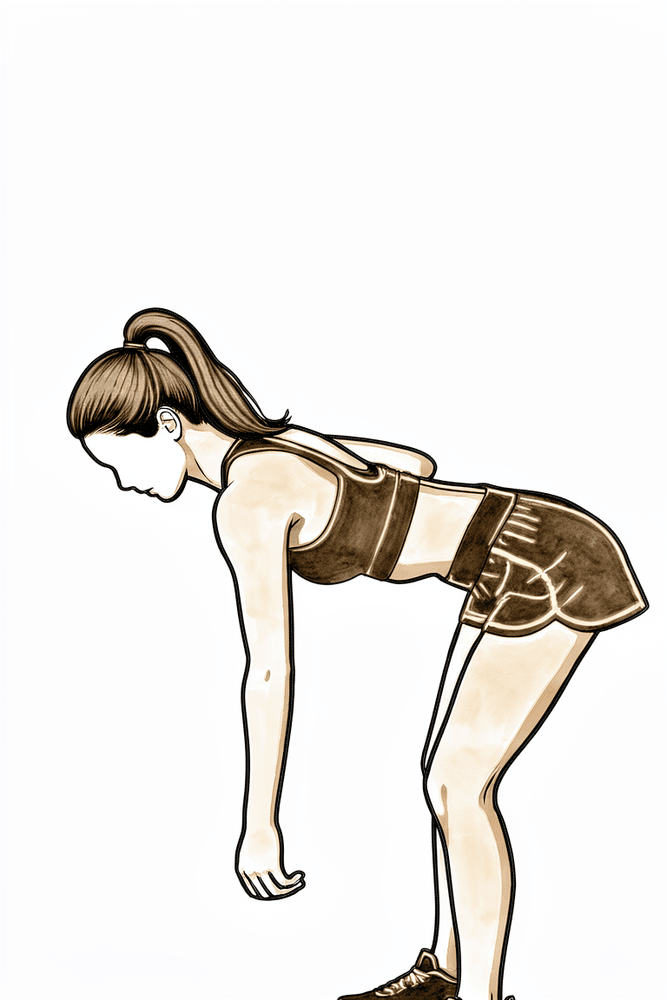
Pendulums
This is a relaxed, passive exercise. Lean forward and let your arm hang and relax down. Use your body to swing the arm gently in small circles, clockwise and anti-clockwise, and to and fro. Let the weight of the arm do the work, with the shoulder muscles relaxed.
About 30 seconds each way, 3 times per day
Kieran Hirpara 4.0
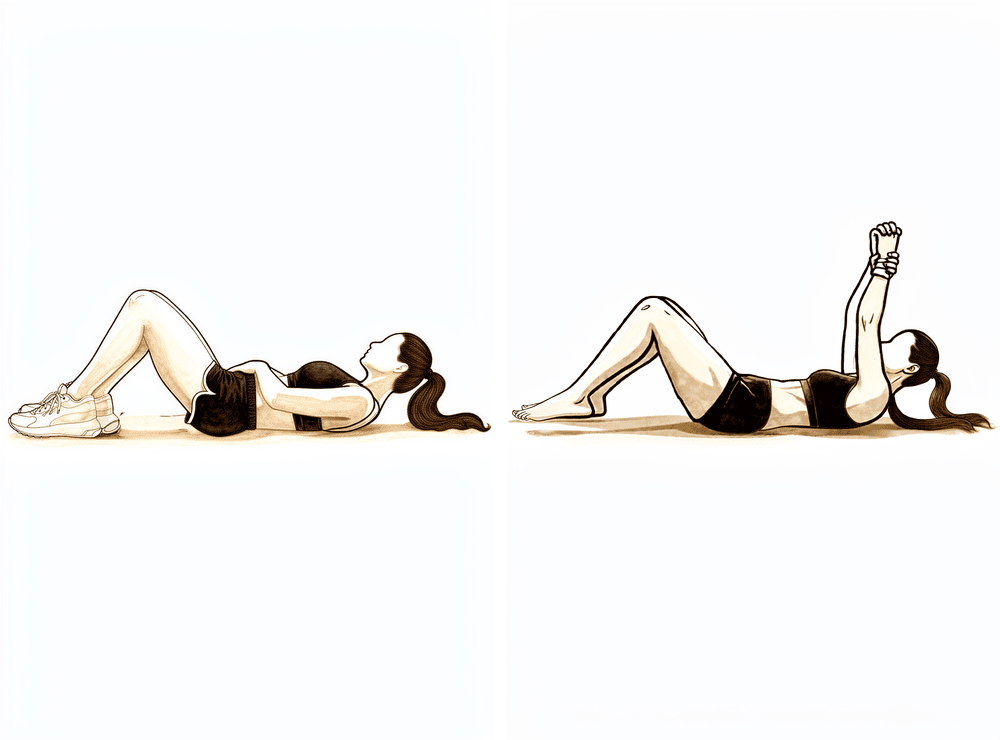
Assisted forward flexion (lying)
If you prefer, lie on your back and hold a stick (or a rolled towel) in both hands. Use your good arm to push the operated arm up over your head, as far as it will comfortably go, then lower it slowly. Push into a firm stretch each time.
10 times, 3 times per day
Kieran Hirpara 4.0
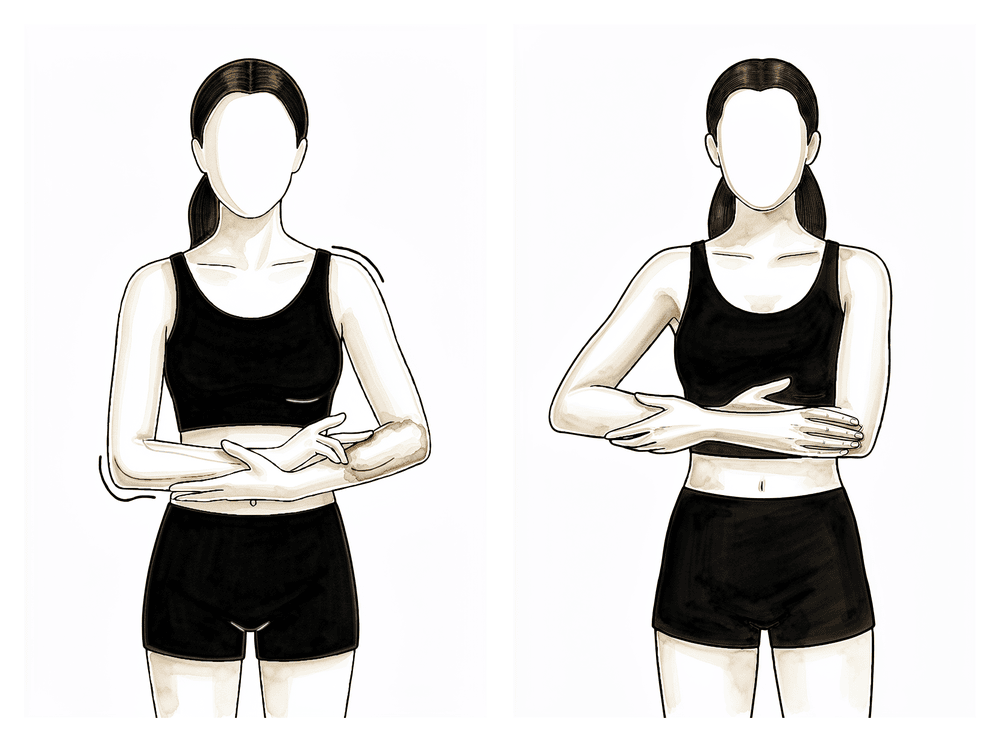
Assisted abduction (cradle)
Cradle the operated arm in your other arm, supporting it under the elbow, and gently rock it out to the side and back, like rocking a baby. Take it to a firm stretch out to the side each time.
10 times, 3 times per day
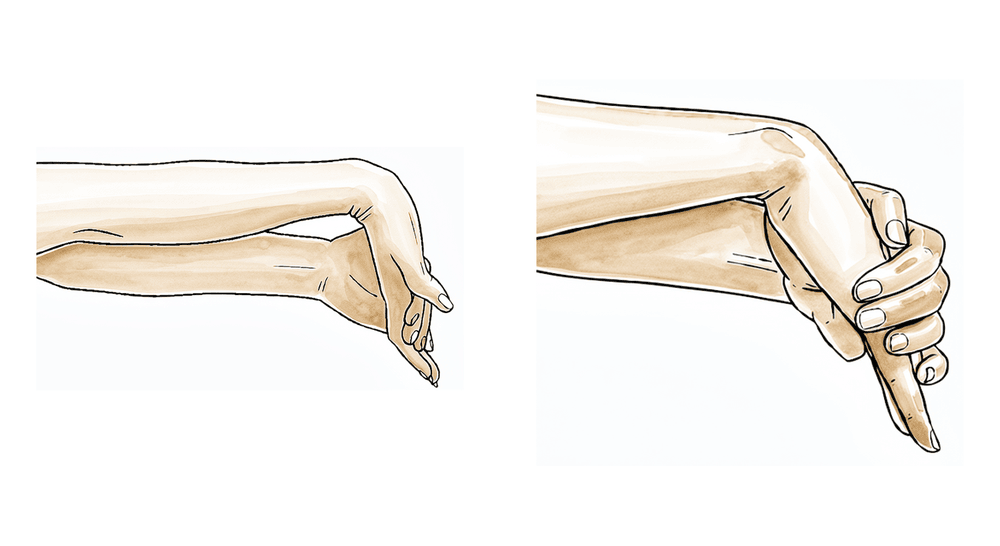
Kieran Hirpara 4.0
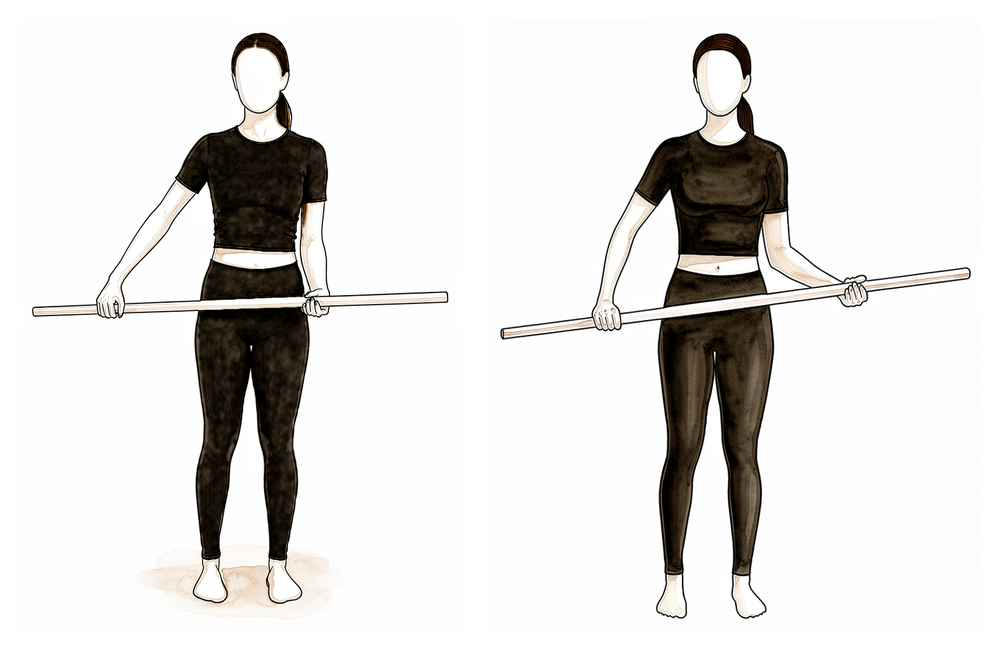
Assisted external rotation with a stick
Lie on your back with your elbow tucked by your side and bent to 90 degrees. Hold a stick in both hands and use your good arm to push the hand of the operated arm outwards, rotating the shoulder. Take it all the way to a firm stretch: there is no limit on how far out you go after this operation, so push the range.
10 times, 3 times per day
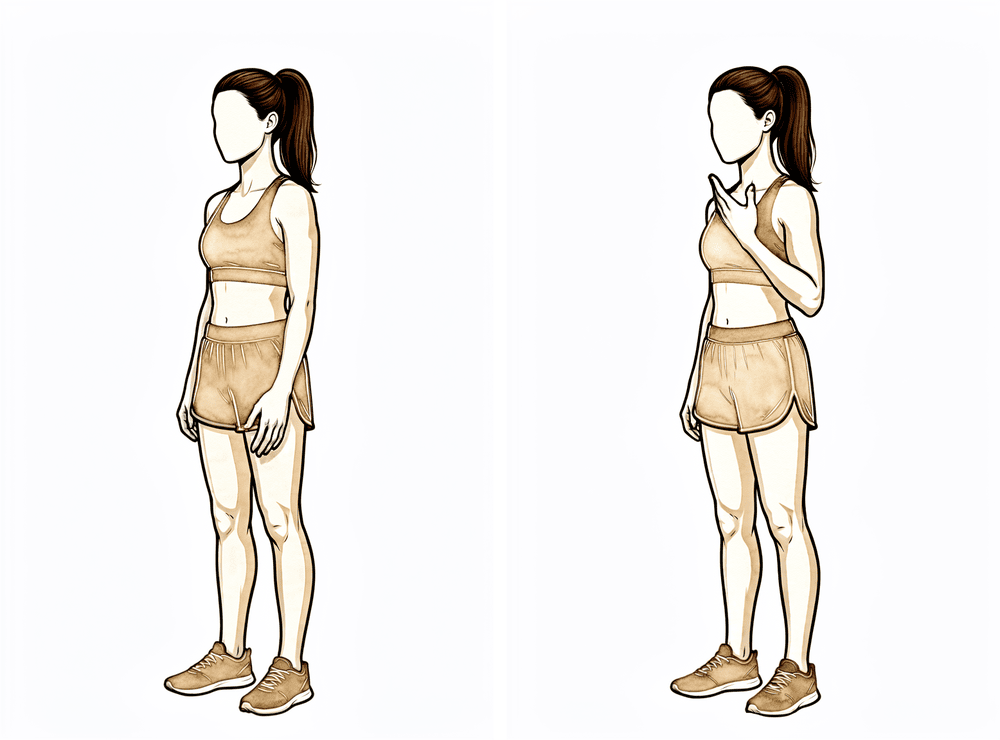
Kieran Hirpara 4.0
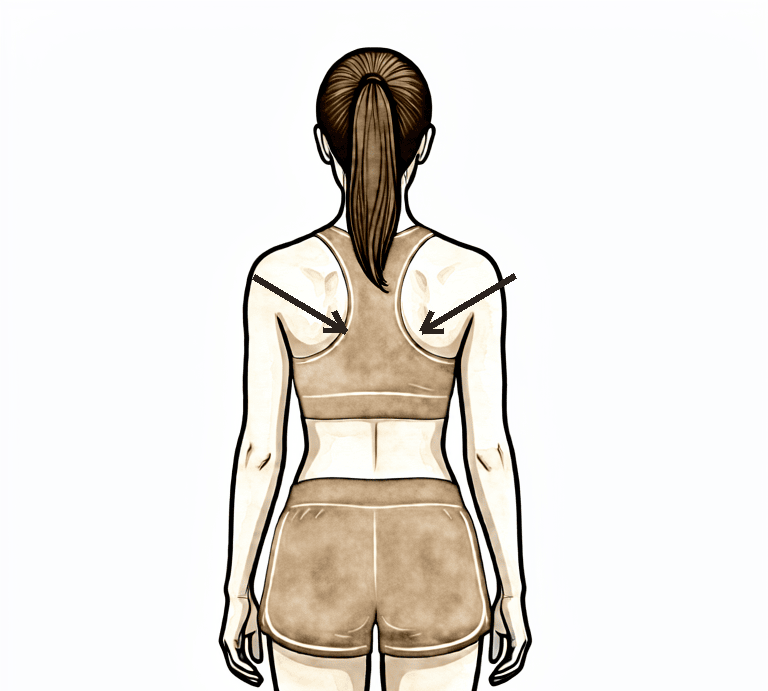
Lower trapezius setting
Squeeze your shoulder blades downwards and together, hold, then relax.
Hold 5 seconds, 5 times; repeat 3 times daily
Kieran Hirpara 4.0
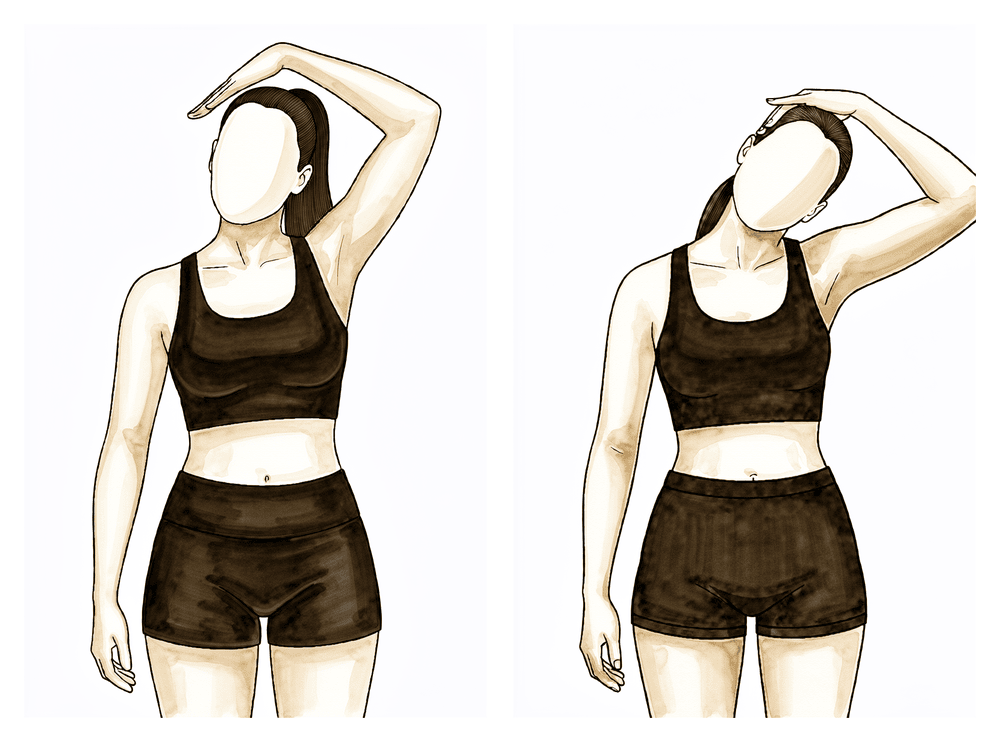
Upper trapezius stretch
Use your good arm to bring your ear gently towards your shoulder, away from the operated side, until you feel a stretch up the side of the neck.
Hold 10 seconds, 3 times; repeat 3 times per day
Kieran Hirpara 4.0
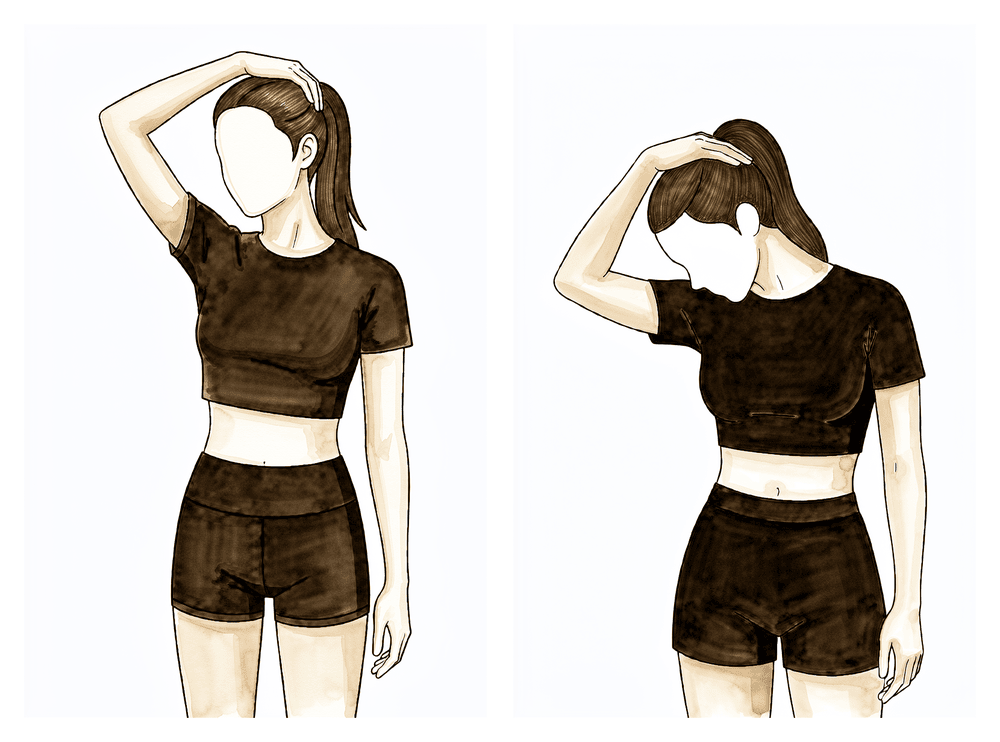
Levator scapulae stretch
Use your good arm to bring your nose down towards your armpit on the opposite side, until you feel a stretch at the base of the neck.
Hold 10 seconds, 3 times; repeat 3 times per day
A physiotherapist will see you in hospital and start you on the exercises below before you go home. These keep the hand, elbow and shoulder moving and begin pushing the shoulder's range straight away. Take your pain relief beforehand so you can move freely. Do them as marked by your team, and carry on with them at home.
Your outpatient rehabilitation¶
After a capsular release, rehabilitation runs in the opposite direction to operations that repair a tendon: there is nothing to protect, so the whole effort goes into keeping the movement. The shoulder is most likely to stiffen up again in the first weeks, so physiotherapy starts straight away, stays frequent, and continues for some months until your range is stable. The phases below follow the pattern of published rehabilitation protocols for this operation (the sources are listed at the end). The week ranges are typical rather than fixed: your physiotherapist will progress you on how your shoulder is moving, not on the calendar.
The journey at a glance:
- Phase I — Early rehabilitation — roughly the first two weeks
- Phase II — Keeping and restoring your range — week 2 to 6
- Phase III — Strengthening — week 6 to 12
- Phase IV — Return to full activity — week 12 onwards
By about three weeks, movement below shoulder height usually becomes more comfortable and most of your range is back, although the arm is often still uncomfortable overhead. By about three months most people find their symptoms have largely settled, and improvement typically continues for six to nine months, sometimes up to a year.
Phase I — Early rehabilitation (Week 0–2)¶
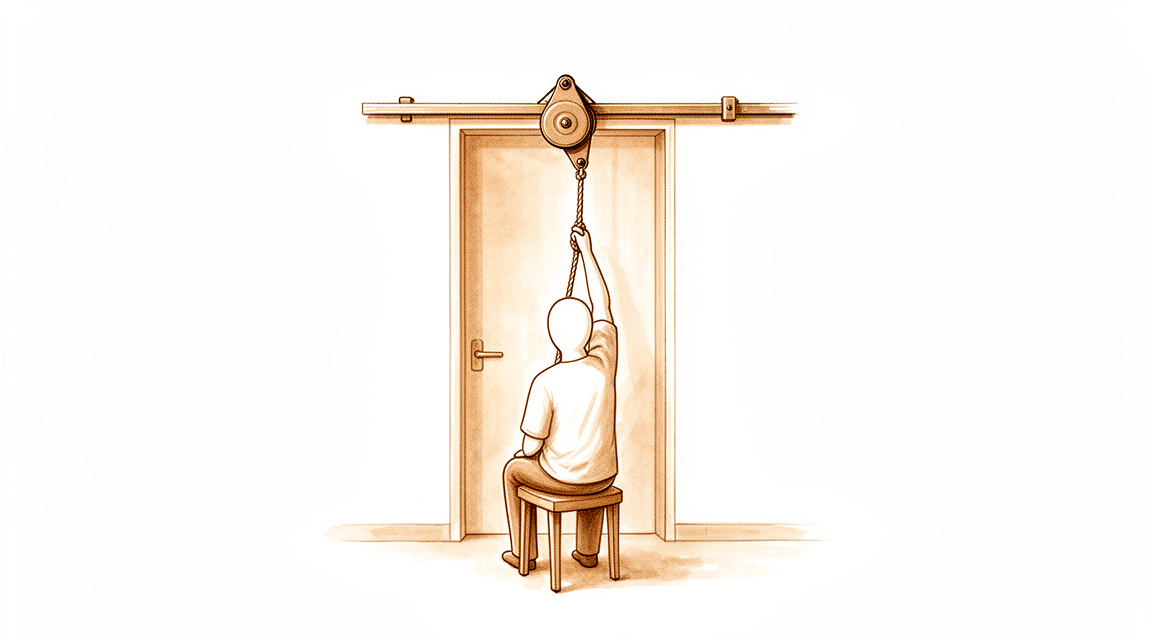
Kieran Hirpara 4.0
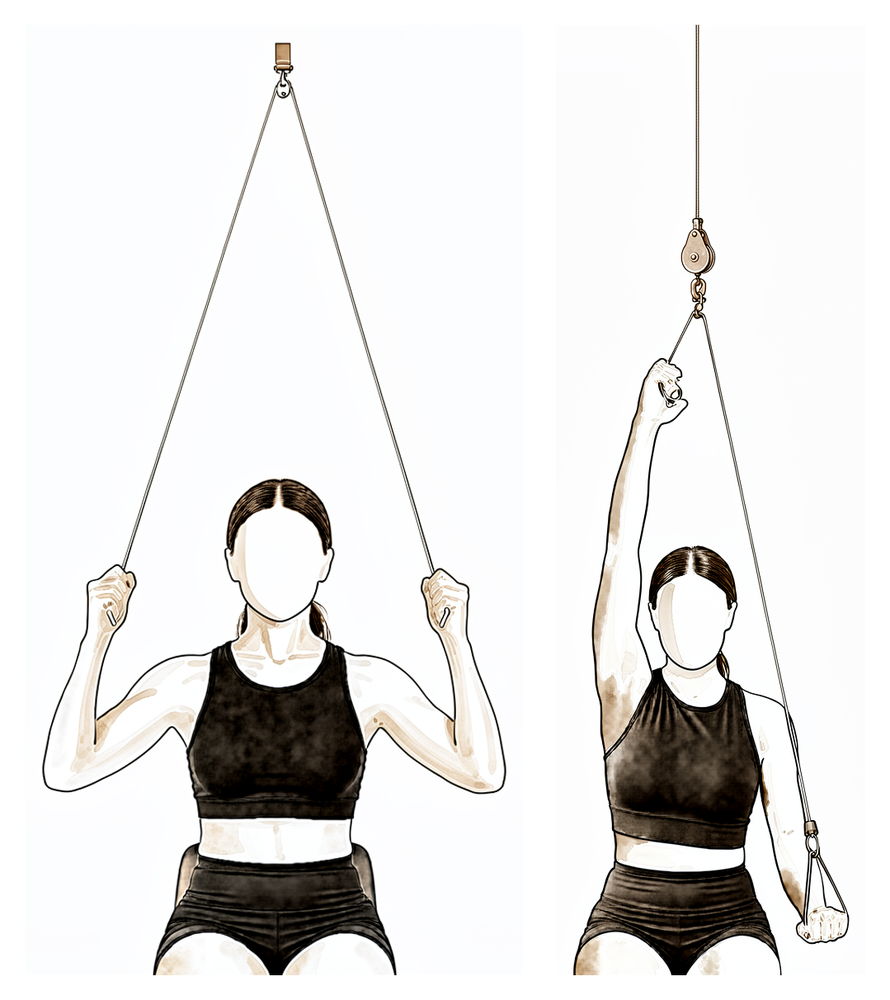
Over-door pulley
Sit under an over-door pulley with a handle in each hand. Pull down with your good arm to raise the operated arm overhead as far as it will go, then lower slowly. Push into a firm stretch each time, not severe pain.
10 times, 3 to 4 times daily
Kieran Hirpara 4.0
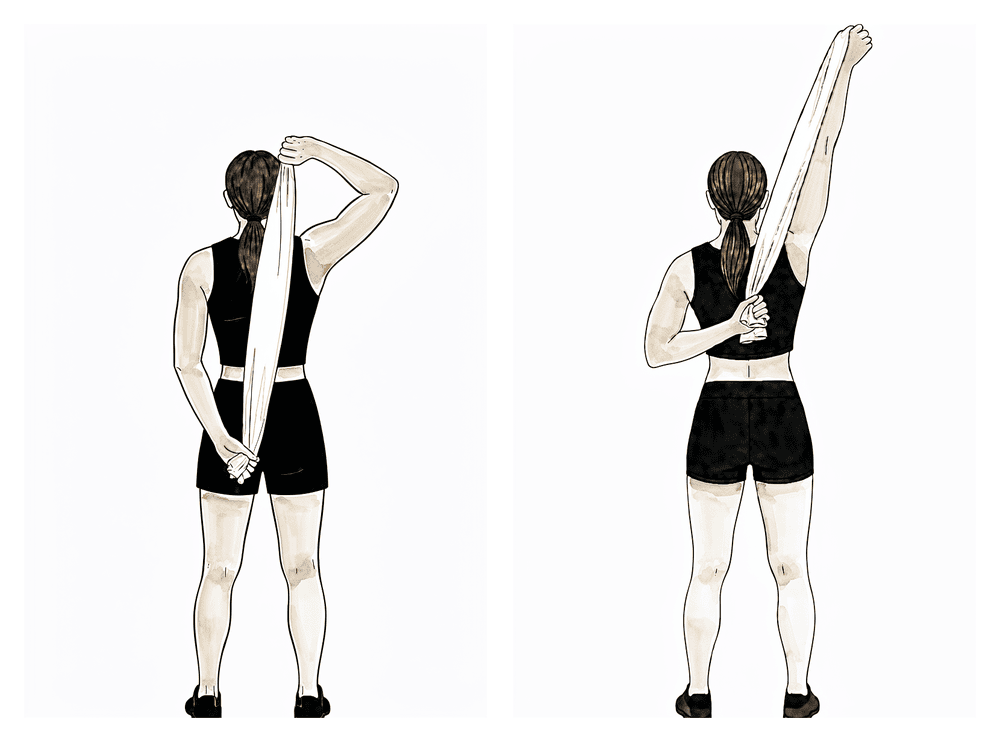
Behind-the-back stretch with a towel
Hold a towel behind your back with the operated hand below, and use your upper hand to draw the lower hand up your back as far as it will go. Take it to a firm stretch, then release: the stretch should ease soon afterwards.
10 times, 3 to 4 times daily
Kieran Hirpara 4.0
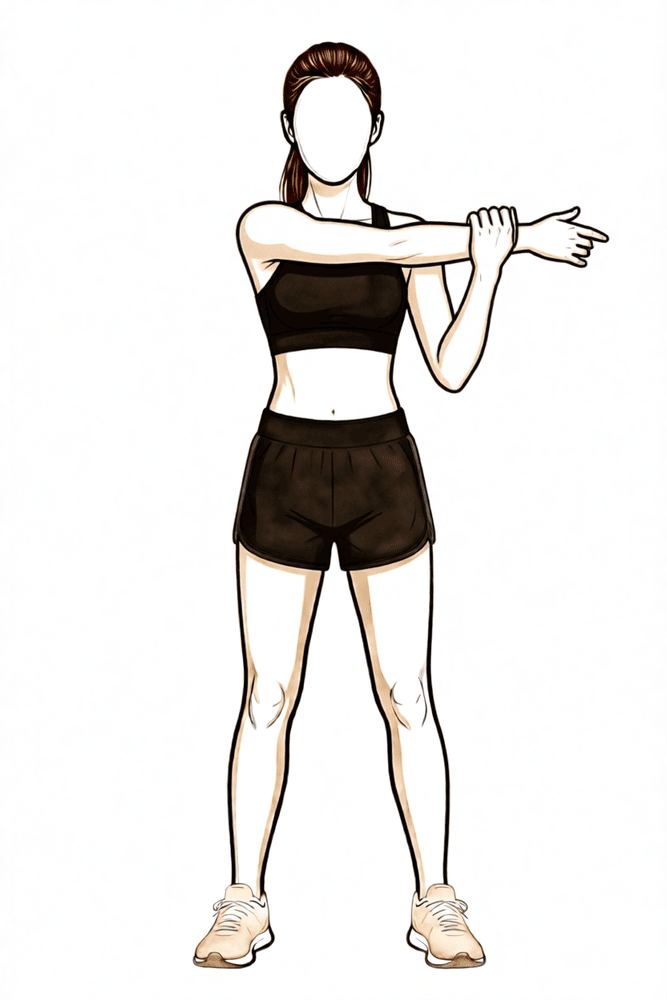
Cross-body stretch
Use your good hand to draw the operated arm across your chest until you feel a firm stretch at the back of the shoulder, then release.
10 times, 3 to 4 times daily
Kieran Hirpara 4.0
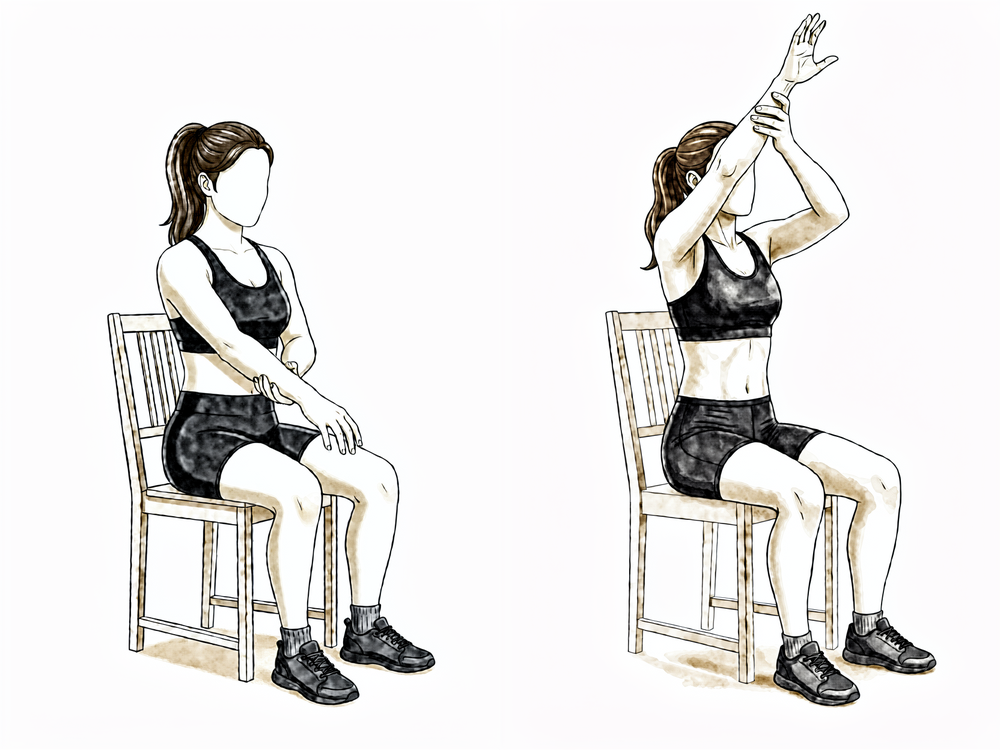
Assisted forward elevation (sitting)
Sitting and leaning forward slightly, support the operated forearm with your good hand and use it to lift the operated arm forwards and up in front of you, as far as is comfortable, then lower it slowly. Let the good arm do the work so the operated shoulder stays relaxed.
As guided by your physiotherapist
The goal of these first two weeks is simple: do not lose the range you gained at surgery. You carry on the hospital exercises at home, several times a day, and add stretches that push the shoulder to its limit in every direction. Good pain control is what makes this possible, so keep taking your pain relief before your exercises and physiotherapy sessions, and use heat before stretching and ice afterwards if it helps. Use the arm for normal light daily activities such as washing, dressing and eating. Push every stretch to the point of firm discomfort, not severe pain, and remember there is no plane you need to hold back from.
Ready for the next phase when… you are doing your home program confidently and independently several times a day, your pain is controlled enough to stretch into the range, and you are holding on to the movement your shoulder had at surgery.
Phase II — Keeping and restoring your range (Week 2–6)¶
Kieran Hirpara 4.0
Wand external rotation (full range)
Continue the stick-assisted external rotation from hospital, now pushing further as the range frees up. With the elbow by your side, rotate the forearm outwards as far as it will go. Keep taking it to its full limit: pushing this range is the whole point of the operation.
10 times, 3 to 4 times daily
Kieran Hirpara 4.0
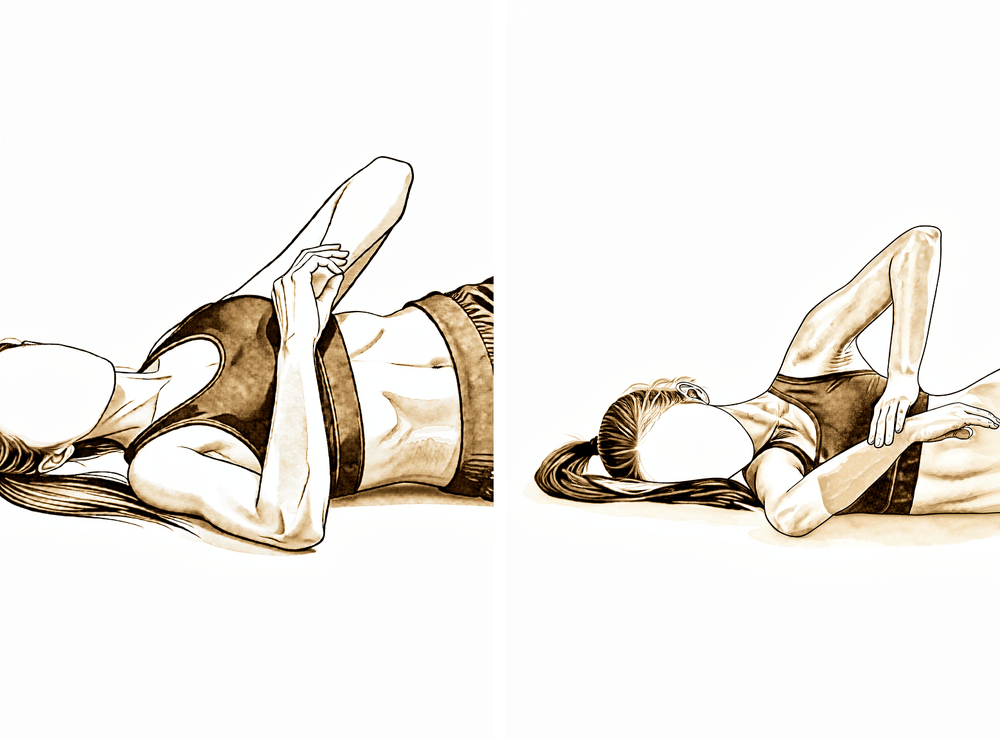
Sleeper stretch
Lie on the operated side with the arm out in front and the elbow bent. Use your good hand to press the forearm down gently towards the bed, until you feel a stretch deep in the shoulder, then ease off.
Hold 20 to 30 seconds, 3 times; 3 to 4 times daily
This phase carries on the frequent physiotherapy and the home stretching program, done several times a day, so the movement won at surgery is not lost and the range keeps building. Your exercises progress from assisted movements towards moving the arm actively in all directions, and your physiotherapist may add hands-on joint mobilisation to help. Keep pushing range in every plane, including external rotation, to its full limit. Use the arm normally for light daily activities.
Ready for the next phase when… the range gained at surgery is being held or is still improving, movement below shoulder height is comfortable, and your pain has settled enough to begin gentle resistance work.
Phase III — Strengthening (Week 6–12)¶
Kieran Hirpara 4.0
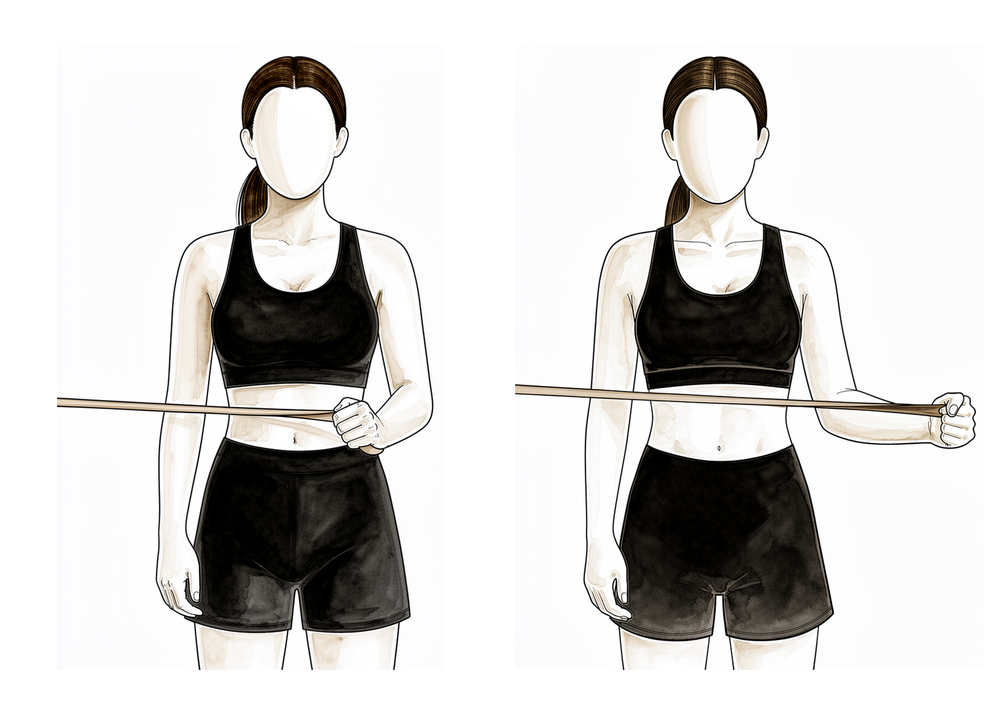
Band external rotation
Stand with your elbow tucked into your side and bent to 90 degrees, holding an elastic band anchored at waist height. Keeping the elbow at your side, rotate the forearm outwards against the band, then return slowly.
2 to 3 sets of 10 to 15, 5 days per week
Kieran Hirpara 4.0
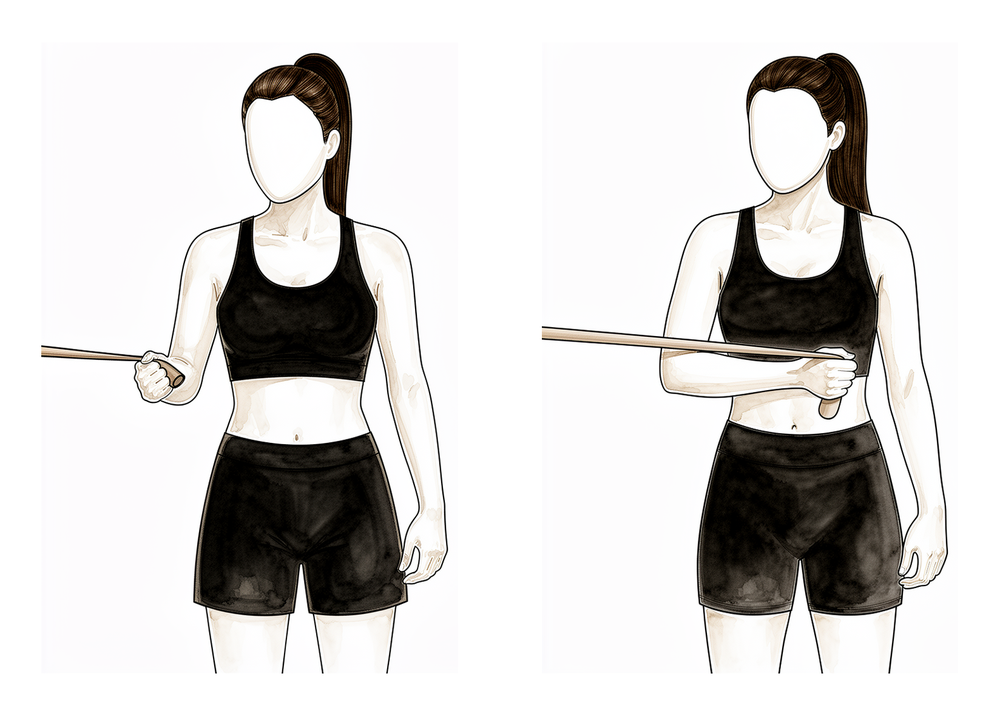
Band internal rotation
With your elbow tucked into your side, hold a band anchored to one side and rotate the forearm inwards across your body against the band, then return slowly.
2 to 3 sets of 10 to 15, 5 days per week
Kieran Hirpara 4.0
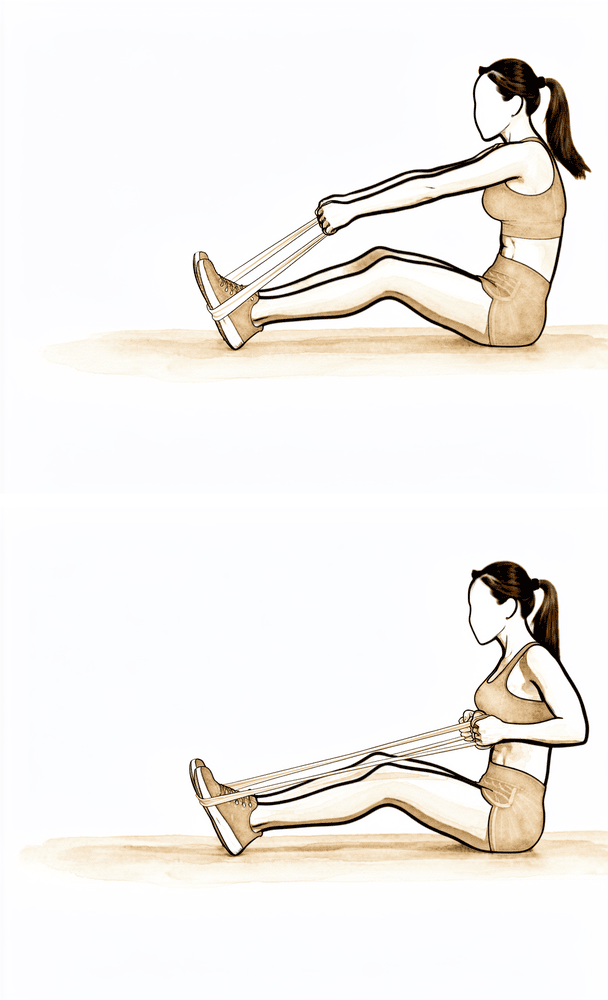
Low row
Hold a band anchored in front of you at waist height. Keeping your arm fairly straight, pull it back and down towards your hip, squeezing the shoulder blade down and back, then return slowly.
2 to 3 sets of 10 to 15, 5 days per week
Kieran Hirpara 4.0
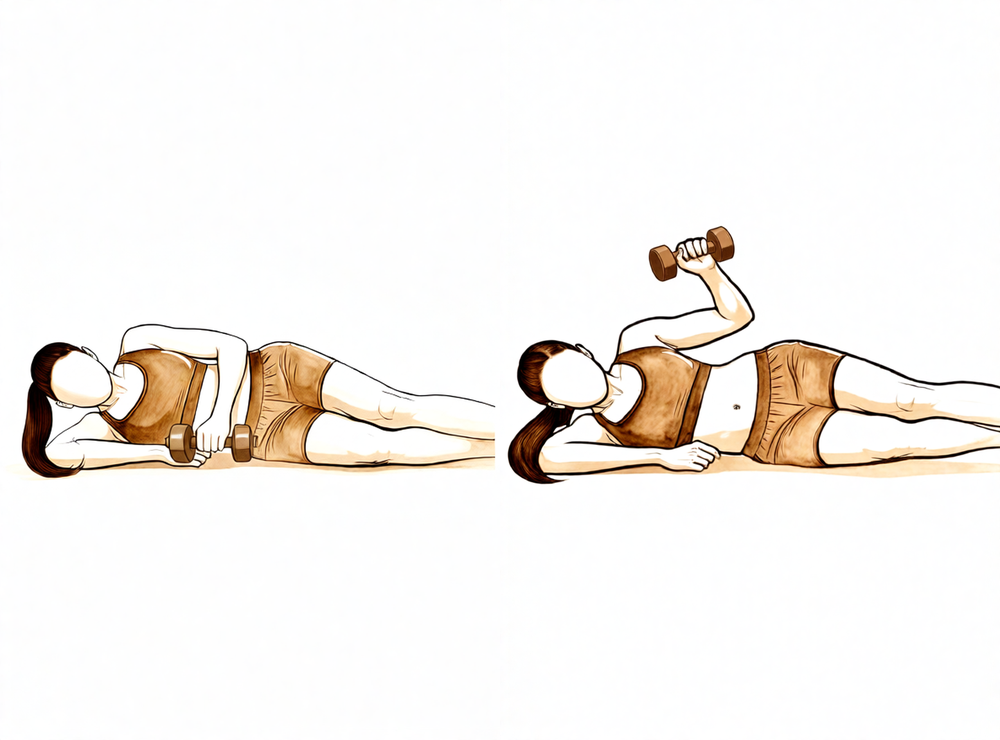
Side-lying external rotation (light weight)
Lie on your good side with the operated elbow bent to 90 degrees and tucked against your side, holding a light weight (about 0.5 to 1.5 kg). Rotate the forearm upwards, then lower slowly: the slow lowering is the important part. Keep the work below shoulder height.
2 to 3 sets of 10 to 15, low load
With your range stable, attention turns to rebuilding the shoulder's strength. Daily stretching continues throughout this phase, because strengthening must never come at the cost of the range you have worked for. Resistance work starts gently, using elastic bands and light weights for the rotator cuff and shoulder-blade muscles, with low loads and higher repetitions. Normal daily activities should be largely back to usual, and lighter recreational activities typically resume during this phase, as guided by your physiotherapist.
Ready for the next phase when… you have full, or near-full, pain-free movement in all directions, and you can manage the strengthening exercises without a flare-up of pain or any loss of range.
Phase IV — Return to full activity (Week 12 onwards)¶
The final phase is a graduated return to heavier work, overhead tasks and sport. Formal rehabilitation usually runs three to four months in total, and the shoulder keeps improving well beyond that: most people continue to gain comfort and confidence for six to nine months, sometimes up to a year. It is worth keeping up a short stretching routine until your range looks after itself without formal exercises. Progression stays guided by how you feel, so if stiffness or pain starts to return, the answer is to ease back and restore the range, not to rest the shoulder.
Returning to activity¶
Most people are back to normal daily activities and to many kinds of work by four to six weeks, because recovery here is driven by keeping your range rather than waiting for tissue to heal. Heavier, more physical work and overhead sport come back gradually over the following weeks to months, as your strength returns. If at any point the shoulder starts to stiffen again, treat it as a signal to push your stretches harder and see your physiotherapist, not to rest.
Your exercises¶
After your protocol¶
The outpatient phases above are adapted from published rehabilitation protocols for arthroscopic capsular release, with recovery milestones drawn from the same sources. The week ranges are typical rather than fixed, and your ongoing rehabilitation is guided individually by your physiotherapist, working with the practice, based on how your shoulder movement recovers. This page works alongside the practice's general recovery advice: see managing post-operative pain and wound care. For the operation itself and the condition it treats, see capsular release and frozen shoulder.
Evidence & references
Adhesive Capsulitis (Frozen Shoulder) — Non-operative Staged Management & Post-operative Rehabilitation (Capsular Release)¶
Topic scope: Both (A) non-operative staged management of primary/secondary adhesive capsulitis (freezing -> frozen -> thawing), including physiotherapy, intra-articular steroid and hydrodilatation; and (B) post-operative rehabilitation after arthroscopic capsular release (ACR).
Defining principle of surgical rehab here (the inversion): Unlike virtually every other shoulder operation -- where a repair (cuff, labrum, pec major, instability) must be protected with a sling and ROM is restricted to avoid disrupting healing tissue -- frozen-shoulder release rehab is the OPPOSITE: the goal is to prevent re-formation of the capsular contracture. So the protocol is immediate, aggressive ROM, usually NO sling, passive + active ROM starting the same day or day 1, with stretching to the end of the freshly gained range. Delay or immobilisation is the enemy (re-stiffening), not the protector. This is the single most important point distinguishing this protocol from the others in this audit.
A. NON-OPERATIVE STAGED MANAGEMENT¶
Natural history / staging (consensus, weak evidence -- descriptive, no RCT)¶
Frozen shoulder is self-limiting in most but typically lasts 12-18 months across 3 clinical stages (Reeves' classic model; staging boundaries overlap and are not sharply separable in practice -- flagged as weak/consensus evidence; the original Reeves model was a single prospective cohort of 49 patients, not an RCT) [Brigham SOC; Chan 2017; Reeves 1975 via Willmore 2020]:
| Stage | Name | Typical duration | Clinical picture | Management emphasis |
|---|---|---|---|---|
| 1 | Freezing (painful/inflammatory) | 2-9 months | Diffuse constant pain, worse at night; progressive ROM loss in a capsular pattern (ER > ABD > flexion > IR); loss of passive ER with arm at side is the hallmark | Pain control; intra-articular steroid; gentle ROM within pain limits -- do NOT force end-range while highly inflamed |
| 2 | Frozen (adhesive/stiff) | 4-12 months | Pain subsides to dull ache; stiffness dominant; marked functional loss | Restore motion: stretching, joint mobilisation grades III-IV, hydrodilatation; consider surgery if recalcitrant |
| 3 | Thawing | 6-9 months (Brigham) | Gradual spontaneous return of motion | Progressive ROM + strengthening; PT 2-3x/week |
(Stage durations from Brigham Standard of Care 2010 and Chan 2017: freezing 2-9 mo, frozen 4-12 mo, thawing 6-9 mo.)
Stepped non-operative interventions¶
- Education / "supervised neglect" + analgesia -- many resolve with reassurance, activity modification and analgesia alone (Codman; Hsu 2011 review). Weak (cohort/expert).
- Physiotherapy -- pendulum, PROM/AAROM/AROM, capsular stretching, joint mobilisation (grades I-II early for pain, III-IV later for tissue extensibility), scapular/posture work. Brigham: PT 1-2x/week in early stages (mainly HEP instruction), 2-3x/week in thawing. PT is best supported as an adjunct to mobilisation/injection/distension, not as a stand-alone cure (Itoi 2016 Current Concepts; Kelley/McClure/Leggin JOSPT 2009 guidance). Moderate; intensity/timing debated. Intensity caveat: end-range/high-intensity stretching is appropriate in the frozen/thawing phase but can be counter-productive in the acutely inflamed freezing phase -- match intensity to irritability (Kelley 2009).
- Intra-articular corticosteroid (glenohumeral) -- superior to placebo and to physiotherapy for short-term (up to 4-12 weeks) pain and function; benefit wanes after ~3 months. Strong for short term (multiple RCTs; Koh 2016 systematic review of 10 RCTs; Cochrane Buchbinder shoulder injection review). BESS pathway: GH steroid recommended for short-term symptom control; long-term (>3 mo) benefit not demonstrated (Rupani/Gwilym BESS 2025). Earlier injection (freezing phase) is the rationale -- steroid targets the inflammatory component.
- Hydrodilatation (distension arthrography) -- distends/ruptures the contracted capsule with saline +/- steroid +/- LA. A controlled, image-guided alternative to surgery. RCT/meta-analytic evidence is mixed: generally produces a transient functional/ROM gain, with no clear superiority over IA steroid alone in several network meta-analyses (Wu 2017 SR/MA of RCTs; Lin 2018 network MA). Some evidence hydrodilatation + steroid > steroid alone in refractory cases (Lee 2017 RCT). Low rate of needing later surgery after distension arthrogram (Nicholson 2020). Moderate; conflicting.
B. POST-OPERATIVE REHABILITATION (the "immediate aggressive ROM" protocols)¶
Surgery is reserved for cases recalcitrant to >=3-6 months of adequate non-operative care (Struyf 2024; Mullen 2025).
Arthroscopic capsular release (ACR)¶
- Controlled, direct-vision release of the contracted capsule (rotator interval, CHL, anterior +/- inferior +/- 360 degree capsulotomy; care re axillary nerve inferiorly). Allows graded release with a low risk of iatrogenic fracture or cuff tear (Kanbe 2018, n=255; Jerosch 2001 360 degree release). Achieves reliable gains in final forward elevation and may shorten recovery (most improved by ~4 months -- McAllister/CORR Insights 2025; Saade 2023 MA favoured ACR for AFE). A gentle, controlled manipulation is often performed as part of the arthroscopic release to confirm the gained range.
Consensus POST-OP phased timeline (applies after arthroscopic capsular release)¶
The hallmark is immediate motion, no protective sling, same-day/day-1 ROM to hold the range just won in theatre.
| Phase | Window | Sling | ROM | Active ROM | Strengthening | Notes |
|---|---|---|---|---|---|---|
| 0 -- Immediate | Day 0-1 (same day) | NO sling (or sling only briefly for comfort/analgesia, discarded fast) | Full passive ROM immediately; PT-assisted forward flexion + ER begun day 1; +/- continuous passive motion (CPM); pendulums; patient does HEP several times/day | AAROM/AROM started day 1 alongside PROM (no protected period) | -- | Intra-articular steroid often injected at time of release to damp post-op inflammatory re-stiffening |
| 1 -- Early | Week 0-2 | None | Aggressive PROM/AAROM to maintain gained range; stretch into end-range daily; hold ER/ABD/flexion | Active motion continued | Light scapular/rotator-cuff activation as pain allows | Pain control critical to allow the patient to move -- adequate analgesia / interscalene block / oral steroid taper |
| 2 -- Strengthening | Week 2-6 | None | Continue to full ROM | Full AROM goal | Rotator cuff + scapular strengthening begins ~week 2 (Kanbe protocol) | Most back to normal daily activity / work by 4-6 weeks |
| 3 -- Return to function | ~6 weeks-3 months | None | Maintain full ROM | Full | Progressive strengthening to full | Recurrence of stiffness is the main failure mode -> continued HEP emphasised |
Representative published protocol (Kanbe 2018, J Orthop Surg Res, n=255, ACR): "passive, assisted-active and stooping (pendulum) exercises for forward flexion and external rotation commenced 1 day after surgery... after 2 weeks of passive exercise, patients began active exercise to strengthen the rotator cuff and scapular stabilisers... after 4-6 weeks patients returned to normal work without limitation." Many ACR series add an intra-articular steroid + controlled manipulation at the index procedure (Filip Struyf 2024; PMC5137660).
Post-surgical physiotherapy is universally agreed to be essential but is under-standardised -- there is no high-level RCT defining the optimal post-release regimen; protocols are consensus/expert and vary widely (Willmore 2020 Shoulder & Elbow, "Post-surgical physiotherapy in frozen shoulder: a review"). Weak/consensus.
KEY CONTROVERSIES¶
- Evidence base for arthroscopic release. ACR gives a controlled, direct-vision release with a low iatrogenic fracture/cuff-tear risk and reliable gains in final elevation. Systematic reviews show consistently acceptable results, though there is no definitive RCT defining the optimal technique (Saade 2023 MA; McAllister 2025). Weak/moderate evidence (large cohorts).
- Steroid timing. Strong short-term benefit (<12 wk) but no durable >3-month benefit; debate over injecting early (freezing/inflammatory phase) vs reserving for refractory cases (Koh 2016; Rupani/Gwilym BESS 2025; Lin 2018).
- Aggressive vs gentle physiotherapy. High-intensity end-range stretching helps in the frozen/thawing phases but may worsen pain and prolong the condition if applied to the acutely inflamed freezing phase -- "intensity should match irritability" (Kelley/McClure 2009; Itoi 2016). Post-operatively, by contrast, aggressive immediate ROM is mandatory to prevent re-stiffening.
- Hydrodilatation worth it? Transient benefit only and not clearly better than IA steroid alone in pooled RCT data (Wu 2017; Lin 2018), though some refractory-case RCT support (Lee 2017) and a low rate of needing later surgery (Nicholson 2020).
- Does anything change the natural history? No intervention is proven to shorten the overall 12-18 month course in the highest-quality reviews; most accelerate symptom relief rather than alter end-point (Rookmoneea 2010 JBJS Br; Hsu 2011). Strong (negative).
EVIDENCE STRENGTH FLAGS (summary)¶
- STRONG (RCT / SR-MA): IA corticosteroid short-term benefit (Koh 2016 SR of 10 RCTs; Cochrane); hydrodilatation = transient, not superior to steroid (Wu 2017 SR-MA of RCTs; Lin 2018 network MA).
- MODERATE: end-range/scapular mobilisation (Yang 2012 RCT); ACR clinical outcomes (large cohorts -- Kanbe 2018 n=255; Jerosch 2001).
- WEAK / CONSENSUS ONLY: 3-stage natural-history model & stage durations (Reeves cohort, descriptive); the post-operative rehab protocol itself (no defining RCT; expert/consensus -- Willmore 2020); optimal ACR technique (published series are heterogeneous).
CITATIONS¶
RAG corpus (180,000+ Orthopaedic articles)¶
- Guyver P, Bruce D, Rees J. Frozen shoulder -- a stiff problem that requires a flexible approach. Maturitas. 2014.
- Kim J, Gahlot N, Park HB. Frozen shoulder: a narrative review of current treatment concepts and the underlying scientific evidence. Clinics in Shoulder and Elbow. 2025;28(4).
- Hsu JE, Anakwenze OA, Warrender WJ, et al. Current review of adhesive capsulitis. J Shoulder Elbow Surg. 2011;20(3):502-514.
- Koh KH. Corticosteroid injection for adhesive capsulitis in primary care: a systematic review of randomised clinical trials. Singapore Med J. 2016.
- Rupani N, Gwilym SE. British Elbow and Shoulder Society patient care pathway: Frozen shoulder. Shoulder & Elbow. 2025;17(4).
- Sheridan MA, Hannafin JA. Upper Extremity: Emphasis on Frozen Shoulder. Orthop Clin North Am. 2006.
- Chan H, Pua P, How C. Physical therapy in the management of frozen shoulder. Singapore Med J. 2017.
- Willmore EG, Millar NL, van der Windt D. Post-surgical physiotherapy in frozen shoulder: a review. Shoulder & Elbow. 2020;14(4).
- Lamplot JD, Lillegraven O, Brophy RH. Outcomes from conservative treatment of shoulder idiopathic adhesive capsulitis... Orthop J Sports Med. 2018.
- Itoi E, Arce G, Bain GI, et al. Shoulder Stiffness: Current Concepts and Concerns. Arthroscopy. 2016;32(7).
- Kanbe K. Clinical outcome of arthroscopic capsular release for frozen shoulder: essential technical points in 255 patients. J Orthop Surg Res. 2018;13(1). (post-op protocol: day-1 ROM, 4-6 wk RTW)
- Jerosch J. 360 degree arthroscopic capsular release in patients with adhesive capsulitis... Knee Surg Sports Traumatol Arthrosc. 2001;9(3).
- McAllister NB. CORR Insights: Releasing forces in adhesive capsulitis... Clin Orthop Relat Res. 2025.
- Saade F, van Rooij F, Saffarini M, et al. Management of shoulder stiffness following rotator cuff repair: a systematic review and meta-analysis. JSES Rev Rep Tech. 2023.
- Wu W, Chang K, Han D, et al. Effectiveness of glenohumeral joint dilatation for treatment of frozen shoulder: a systematic review and meta-analysis of RCTs. Sci Rep. 2017. (SR-MA of RCTs)
- Lin M, Hsiao M, Tu Y, et al. Comparative efficacy of intra-articular steroid injection and distension... a systematic review and network meta-analysis. Arch Phys Med Rehabil. 2018. (network MA)
- Lee D, Yoon S, Lee MY, et al. Capsule-preserving hydrodilatation with corticosteroid vs corticosteroid alone in refractory adhesive capsulitis: a randomized controlled trial. Arch Phys Med Rehabil. 2017. (RCT)
- Nicholson JA, Slader B, Martindale A, et al. Distension arthrogram in the treatment of adhesive capsulitis has a low rate of repeat intervention. Bone Joint J. 2020;102-B(5).
- Uppal HS. Frozen shoulder: a systematic review of therapeutic options. World J Orthop. 2015.
- Mullen JP, Hauer TM, Lau EN, et al. Adhesive capsulitis of the shoulder. Arthroscopy. 2025;41(7).
- Yang J, Jan M, Chang C, et al. Effectiveness of the end-range mobilization and scapular mobilization approach... a randomized control trial. Manual Therapy. 2012. (RCT)
- Rookmoneea M, et al. The effectiveness of interventions in the management of patients with primary frozen shoulder. J Bone Joint Surg Br. 2010;92-B(9).
- Struyf F. Frozen Shoulder. 2024 (surgical indication & post-op steroid + controlled manipulation).
Published rehab protocols (URLs)¶
- Brigham & Women's Hospital -- Standard of Care: Shoulder Adhesive Capsulitis (Dept of Rehabilitation Services, 2010): https://www.brighamandwomens.org/assets/BWH/patients-and-families/rehabilitation-services/pdfs/shoulder-adhesive-capsulitis.pdf (source for the 12-18 mo / 3-stage durations, capsular pattern, PT frequency 1-2x/wk early & 2-3x/wk thawing, mobilisation grades, steroid 4-6 wk short-term benefit).
- BESS (British Elbow & Shoulder Society) Frozen Shoulder patient care pathway -- Rupani & Gwilym, Shoulder & Elbow 2025 (GH steroid short-term only, no >3 mo benefit).
- Kanbe 2018 ACR open-access (post-op day-1 ROM protocol): https://pmc.ncbi.nlm.nih.gov/articles/PMC5857121/
- ChoosePT / APTA patient guide to frozen shoulder (lay phased overview): https://www.choosept.com/guide/physical-therapy-guide-frozen-shoulder-adhesive-capsulitis