Boutonnière Deformity PDF Evidence¶
Extensor central-slip injury at the middle finger joint; early splinting prevents the zigzag deformity, established cases need surgery.
What you're feeling¶
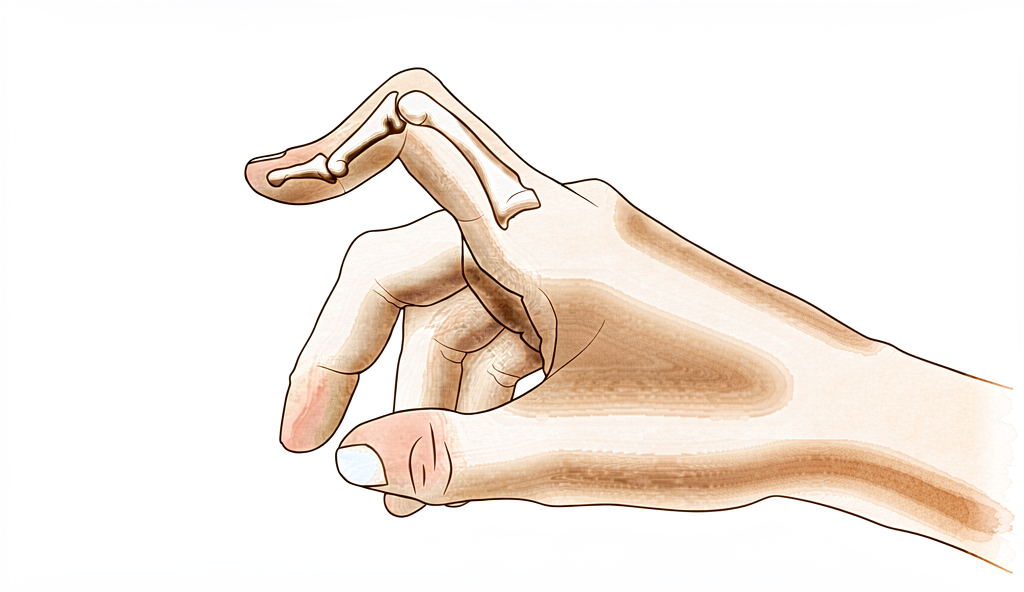
You may notice your middle finger joint bends inward while the tip joint sticks out. This specific shape is called a boutonniere deformity. It happens when the tendons on top of your finger slip out of place. You might see this change develop slowly over time, or it may appear suddenly after an injury.
Pain often centers around the middle joint of your finger. The discomfort can feel like a deep ache or a sharp sting when you move the finger. You might find that bending the finger fully causes more pain than keeping it straight. Activities that require gripping or pinching can become difficult. Simple tasks like buttoning a shirt, turning a doorknob, or typing may feel awkward or painful.
Your finger may feel stiff, especially in the morning. You might notice swelling around the middle joint. This stiffness can make it hard to make a fist. If you have rheumatoid arthritis, the deformity may progress differently than if it came from trauma. Without arthritis or injury, about 13% of people experience this condition.
The tip of your finger might also feel unstable. In some cases, the tip joint bends downward more than usual. This can make it hard to rest your finger flat on a table. You may struggle to push open heavy doors or lift light objects with that hand. Sleeping on your side might press against the deformed finger, causing discomfort.
It is important to distinguish this true deformity from a similar-looking injury called pseudoboutonniere. The two conditions require different care. Your surgeon will look closely at how your finger moves to tell them apart. Understanding exactly what you are feeling helps guide the best treatment plan for you.
What's actually happening¶
Your finger joint is a complex hinge made of bones, tendons, and a protective sleeve called the joint capsule. In a healthy finger, a central tendon runs straight down the middle of your finger to help it straighten. This tendon acts like the main rope pulling your finger open.
In Boutonnière deformity, that central tendon is damaged or weakened. It might be torn from trauma or stretched out by conditions like rheumatoid arthritis. When this central support fails, the balance of forces in your finger changes. The side tendons, which usually help bend the finger, start to pull too hard.
Think of it like a zipper that has come off track. The parts are still there, but they are no longer sliding smoothly together. Because the central tendon is not holding things in place, the side tendons slip to the sides. This causes the middle joint of your finger to bend inward, while the tip joint may stick out.
This shift in tension is why your finger looks crooked and feels stiff. The joint capsule, which normally keeps the joint stable, becomes tight and unbalanced. Over time, the tissues adapt to this new, incorrect position. This is why the deformity can persist even after you try conservative treatments like splinting or therapy.
The most important factor in this problem is the change in your tendons and related structures. These changes happen early, which is why accurate diagnosis is critical. Your surgeon needs to distinguish between a true Boutonnière deformity and a similar issue called pseudoboutonniere injury. The treatment path depends entirely on getting this distinction right.
If the damage is caught early, your surgeon may focus on restoring the central tendon’s position. In some cases, they might use a small piece of another tendon to rebuild the central slip. This new graft mimics the original tendon’s function while keeping other finger movements intact. The goal is to keep the joint centered and stable so you can move it again.
However, if the deformity has been present for a long time, the tissues may have changed permanently. In these chronic cases, simple repairs might not work. The natural history of this condition often leads to persistent issues, especially if rheumatoid arthritis is involved. Long-term results for soft tissue reconstruction in these cases can be unreliable. Sometimes, a more definitive salvage procedure is needed to correct the shape and function of your finger.
What we can do about it¶
We start with non-surgical care to restore movement. You will try serial casting for adequate extension. This is followed by three months of relative motion flexion orthotic use. Your surgeon may also recommend physiotherapy. One to two grades of range of motion improvement can be achieved with nonoperative treatment. However, deformity can persist even after dedicated conservative management. We use relative motion flexion orthoses to increase active distal interphalangeal joint flexion. This helps improve your middle finger joint extension. You must give this approach time to work before considering surgery.
Medical management focuses on comfort and inflammation. If your deformity is linked to rheumatoid arthritis, we address the underlying disease activity. Pain medication and anti-inflammatories help manage discomfort. Injections may be offered to reduce swelling in the joint. These treatments aim to keep the joint mobile and pain-free while you undergo therapy. The goal is to stabilize the condition and improve your daily function without an operation.
Surgery is considered when conservative care has reached its limit. We differentiate a true boutonniere deformity from a pseudoboutonniere injury before deciding. This distinction is critical in determining clinical management. A successful operative result depends on complete preoperative examination, correct staging of the deformity, and proper timing of treatment. If soft tissue reconstruction is needed, we understand that long-term results can be unreliable. Recurrent or persistent deformity is best treated with a salvage procedure. In some cases, a Y-shaped tendon graft provides good or excellent results. Your surgeon will determine the true etiology before surgical intervention. This ensures the chosen procedure matches your specific anatomy and needs.
What to expect¶
Your outlook depends heavily on whether this is a true deformity or a similar injury called a pseudoboutonniere. Your surgeon must confirm the diagnosis first because the treatment path changes completely based on that distinction. If you have rheumatoid arthritis, long-term results from soft tissue repair are often unreliable. In these cases, persistent or recurring deformity may require a salvage procedure later on.
For most people without rheumatoid arthritis, the condition does not always resolve on its own. Nonoperative treatment can improve your range of motion by one to two grades. However, the visible deformity may persist even after you complete dedicated conservative management. If conservative care is not enough, surgery offers a strong option. A Y-shaped tendon graft provides good or excellent results in 16 of 18 patients in reported series. Success also relies on your surgeon performing a complete examination, staging the deformity correctly, and choosing the right time for intervention.
Recovery is a gradual process. If you start with nonoperative care, you might use serial casting to straighten the finger, followed by three months of relative motion flexion orthotic use. This approach yields similar results to other methods for chronic cases and is typically attempted before considering surgery. You should expect to wear an orthosis for several months to maintain extension and improve flexion.
If surgery is needed, the goal is to restore function and alignment. You will need to follow your surgeon’s specific instructions closely. The natural history of this deformity can vary, but early and accurate management leads to the best outcomes. Be patient with the healing process. It takes time for tendons and joints to adapt to their new positions. Your surgeon will guide you through each stage to ensure the best possible return to your daily activities.
When to see someone¶
See your GP if you notice a bend in the middle joint of your finger that does not straighten. Ask for a specialist review if you have persistent pain that does not improve with rest. Seek care if you feel weakness or instability in the finger. Go to a doctor if the finger locks or gives way during use. Contact your surgeon if symptoms interfere with your sleep or work. Sudden worsening of the deformity also requires prompt attention. Accurate diagnosis is critical for proper treatment. Differentiating a true deformity from a similar injury helps determine the right care. Early evaluation ensures the best outcome for your hand function.
Evidence & references
title: "Boutonnière Deformity" slug: boutonniere-deformity region: hand audience: patient mesh_terms: ["Finger Joint", "Hand Deformities, Acquired", "Finger Injuries", "Metacarpophalangeal Joint", "Arthritis, Rheumatoid", "Tendons", "Orthotic Devices", "Joint Prosthesis"] article_count: 137 model_used: Qwen3.6-35B-A3B-Q8_0.gguf generated_at: '2026-06-13T10:01:18+00:00' key_articles: - title: "The relative motion concept in acute and chronic boutonniere deformity: Invited commentary" ref_num: 1 evidence_tier: paper evidence_level: 4 doi: 10.1016/j.jht.2023.02.005 year: 2023 - title: "Boutonniere Versus Pseudoboutonniere Deformities: Pathoanatomy, Diagnosis, and Treatment" ref_num: 2 evidence_tier: paper evidence_level: 5 doi: 10.1016/j.jhsa.2022.10.019 year: 2023 - title: "Correction of the Rheumatoid Boutonnière Deformity" ref_num: 3 evidence_tier: paper evidence_level: 4 doi: 10.2106/00004623-196951070-00009 year: 1969 - title: "Posttraumatic Boutonnière and Swan Neck Deformities" ref_num: 4 evidence_tier: paper evidence_level: 5 doi: 10.5435/jaaos-d-14-00272 year: 2015 - title: "Thumb boutonnière deformity without rheumatoid arthritis or trauma" ref_num: 5 evidence_tier: paper evidence_level: 3 doi: 10.1177/1753193417704610 year: 2017 - title: "Y-Shaped Tendon Graft—A Technique in the Reconstruction of Posttraumatic Chronic Boutonniere Deformity" ref_num: 6 evidence_tier: paper evidence_level: 4 doi: 10.1016/j.jhsa.2021.01.003 year: 2021 - title: "Fractional Fowler Tenotomy for Chronic Mallet Finger: A Cadaveric Biomechanical Study" ref_num: 7 evidence_tier: paper evidence_level: 5 doi: 10.1016/j.jhsa.2012.07.039 year: 2012 - title: "Nonoperative treatment of the Boutonniere deformity: Is there a difference in outcomes?" ref_num: 8 evidence_tier: paper evidence_level: 3 doi: 10.1016/j.jht.2025.02.013 year: 2025 - title: "Treatment of Boutonniere Finger Deformity in Rheumatoid Arthritis" ref_num: 9 evidence_tier: paper evidence_level: 5 doi: 10.1016/j.jhsa.2011.05.029 year: 2011 - title: "Operative Correction of Swan-Neck and Boutonniere Deformities in the Rheumatoid Hand" ref_num: 10 evidence_tier: paper evidence_level: 5 doi: 10.5435/00124635-199903000-00002 year: 1999 - title: "Metacarpophalangeal Joint Arthroplasty in Rheumatoid Arthritis" ref_num: 11 evidence_tier: paper evidence_level: 5 doi: 10.5435/00124635-200305000-00005 year: 2003 - title: "Clarification of Extensor Tenotomy for Finger Deformities" ref_num: 12 evidence_tier: paper evidence_level: 5 doi: 10.1016/j.jhsa.2022.07.008 year: 2022 - title: "The Use of Relative Motion Flexion Orthoses for Chronic Boutonniere Deformity" ref_num: 13 evidence_tier: paper evidence_level: 4 doi: 10.1016/j.jhsa.2022.08.007 year: 2024 - title: "Swan Neck Deformity after Distal Interphalangeal Joint Flexion Contractures: A Biomechanical Analysis" ref_num: 14 evidence_tier: paper evidence_level: 5 doi: 10.1016/j.jht.2009.11.005 year: 2010 - title: "Finger Metacarpophalangeal Joint Injuries in Athletes: Evaluation, Diagnosis, Treatment, and Return to Play" ref_num: 15 evidence_tier: paper evidence_level: 5 doi: 10.5435/jaaos-d-21-01031 year: 2023 - title: "A modified Terrono classification for Type 1 thumb deformity in rheumatoid arthritis: a cross-sectional analysis" ref_num: 17 evidence_tier: paper evidence_level: 3 doi: 10.1177/1753193419886719 year: 2019 - title: "An in-depth look at zone III and IV anatomy of the finger extensor mechanism and some clinical implications for use of the relative motion flexion orthosis" ref_num: 19 evidence_tier: paper evidence_level: 5 doi: 10.1016/j.jht.2023.01.002 year: 2023 - title: "Finger Deformities Caused by Rheumatoid Arthritis" ref_num: 21 evidence_tier: paper evidence_level: 4 doi: 10.2106/00004623-195739030-00006 year: 1957 - title: "Reconstruction of the Extensor Central Slip Using a Distally Based Flexor Digitorum Superficialis Slip" ref_num: 24 evidence_tier: paper evidence_level: 4 doi: 10.1016/j.jhsa.2009.01.025 year: 2009 - title: "Complications of Proximal Interphalangeal Joint Injuries" ref_num: 33 evidence_tier: paper evidence_level: 5 doi: 10.1016/j.hcl.2017.12.014 year: 2018 - title: "Visual detection of cortical breaks in hand joints: reliability and validity of high-resolution peripheral quantitative CT compared to microCT" ref_num: 37 evidence_tier: paper evidence_level: 4 doi: 10.1186/s12891-016-1148-y year: 2016 synthesis_version: "v2" verifier_status: skipped
Overview¶
- Differentiating a true boutonniere deformity from a pseudoboutonniere injury is critical in determining clinical management [2].
- An understanding of the anatomy, clinical presentation, treatment options, and expected outcomes is crucial for optimal treatment of posttraumatic boutonniere and swan neck deformities [4].
- The natural history of the boutonnière deformity in rheumatoid arthritis is outlined, and a simple method of repair is described [3].
- The prevalence of boutonnière deformity without rheumatoid arthritis or trauma is approximately 13% [5].
- One to two grades of ROM improvement can be achieved with nonoperative treatment, although deformity can persist even after dedicated conservative management [8].
- Similar results occurred for chronic boutonniere deformity using serial casting for adequate extension followed by 3 months of RMF orthotic use, which should be attempted prior to surgical intervention [1].
- Long-term results following soft tissue reconstruction for boutonniere deformity in rheumatoid arthritis are unreliable, and recurrent or persistent deformity is best treated with a salvage procedure [9].
- A successful operative result for swan-neck and boutonniere deformities in the rheumatoid hand depends on complete preoperative examination, correct staging of the deformity, and proper timing of treatment [10].
- The Y-shaped tendon graft can be a useful procedure for the correction of chronic boutonniere deformity, providing good or excellent results in 16 of 18 patients in one series [6].
- Detachment of up to two-thirds of the phalangeal length was effective in reducing extensor lag of the DIP joint and did not cause any boutonniere deformity in a cadaveric model of fractional Fowler tenotomy for chronic mallet finger [7].
Anatomy & Pathophysiology¶
- Boutonnière deformity can persist even after dedicated conservative management [8].
- One to two grades of range of motion improvement can be achieved with nonoperative treatment of Boutonnière deformity [8].
- Accurate diagnosis and treatment of finger metacarpophalangeal joint injuries begins with an understanding of all potential diagnoses [15].
- Hand surgery and hand therapy practice interventions, including use of relative motion flexion orthoses for management of non-surgical and surgical extensor mechanism injuries, may benefit from an in-depth look at extensor mechanism zone III and IV anatomy and biomechanics [19].
- The most important factor in the development of finger deformities is the changes occurring in the tendons and related structures, especially in early stages [21].
- Reconstruction of the extensor central slip using a distally based flexor digitorum superficialis slip provides a robust repair that anatomically mimics the extensor central slip while maintaining the function of the donor FDS tendon [24].
- The main goals of any treatment of a proximal interphalangeal joint complication are maintaining concentric reduction of the joint, restoring joint stability, and facilitating early range-of-motion exercises [33].
Classification¶
- Differentiating a true boutonniere deformity from a pseudoboutonniere injury is critical in determining clinical management [2].
- The natural history of the boutonnière deformity in rheumatoid arthritis is outlined [3].
- The prevalence of boutonnière deformity without rheumatoid arthritis or trauma is approximately 13% [5].
- A modified Terrono classification for Type 1 thumb deformity in rheumatoid arthritis could detect advanced deformity earlier and was more strongly correlated with hand function [17].
Clinical Presentation¶
- Differentiating a true boutonniere deformity from a pseudoboutonniere injury is critical in determining clinical management [2].
- An understanding of the clinical presentation is crucial for optimal treatment of posttraumatic boutonnière and swan neck deformities [4].
- Accurate diagnosis of finger metacarpophalangeal joint injuries begins with an understanding of all potential diagnoses [15].
- The natural history of the boutonnière deformity in rheumatoid arthritis is outlined in historical literature [3].
- The prevalence of boutonnière deformity without rheumatoid arthritis or trauma is approximately 13% [5].
- The swan neck deformity can progress significantly with time due to increasing distal interphalangeal joint flexion contracture [14].
Investigations¶
- Differentiating a true boutonniere deformity from a pseudoboutonniere injury is critical in determining clinical management [2].
- An understanding of the anatomy, clinical presentation, treatment options, and expected outcomes is crucial for optimal treatment of posttraumatic boutonnière and swan neck deformities [4].
- Accurate diagnosis and treatment of finger metacarpophalangeal joint injuries begins with an understanding of all potential diagnoses [15].
- It is necessary to determine the true etiology before surgical intervention [12].
- A successful operative result depends on complete preoperative examination, correct staging of the deformity, and proper timing of treatment [10].
- Cortical breaks were commonly visualized in MCP and PIP joints with HR-pQCT and microCT [37].
Treatment¶
- Serial casting for adequate extension followed by 3 months of relative motion flexion (RMF) orthotic use should be attempted prior to surgical intervention for chronic boutonniere deformity [1].
- Differentiating a true boutonniere deformity from a pseudoboutonniere injury is critical in determining clinical management [2].
- A simple method of repair is described for the boutonnière deformity in rheumatoid arthritis [3].
- Understanding the anatomy, clinical presentation, treatment options, and expected outcomes is crucial for optimal treatment of posttraumatic boutonnière and swan neck deformities [4].
- The prevalence of boutonnière deformity without rheumatoid arthritis or trauma is approximately 13% [5].
- The Y-shaped tendon graft is a useful procedure for the correction of chronic boutonniere deformity, providing good or excellent results in 16 of 18 patients in a reported series [6].
- Detachment of up to two-thirds of the phalangeal length is effective in reducing extensor lag of the DIP joint and does not cause any boutonniere deformity in a cadaveric model [7].
- One to two grades of ROM improvement can be achieved with nonoperative treatment, although deformity can persist even after dedicated conservative management [8].
- Long-term results following soft tissue reconstruction for boutonniere deformity in rheumatoid arthritis are unreliable, and recurrent or persistent deformity is best treated with a salvage procedure [9].
- A successful operative result for swan-neck and boutonniere deformities in the rheumatoid hand depends on complete preoperative examination, correct staging of the deformity, and proper timing of treatment [10].
- Metacarpophalangeal joint arthroplasty improves function and deformity and achieves nearly uniform patient satisfaction in rheumatoid arthritis [11].
- One technique does not treat all finger deformities uniformly, highlighting the need to determine the true etiology before surgical intervention [12].
- The use of relative motion flexion orthoses (RMFO) is effective in increasing active distal interphalangeal joint flexion and improving PIP extension in patients with Burton stage 1 chronic boutonniere deformity [13].
Complications¶
- Differentiating a true boutonniere deformity from a pseudoboutonniere injury is critical in determining clinical management [2].
- The prevalence of boutonniere deformity without rheumatoid arthritis or trauma is approximately 13% [5].
- Detachment of up to two-thirds of the phalangeal length was effective in reducing extensor lag of the DIP joint and did not cause any boutonniere deformity in a cadaveric model [7].
- Long-term results following soft tissue reconstruction for boutonniere finger deformity in rheumatoid arthritis are unreliable [9].
- Recurrent or persistent deformity is best treated with a salvage procedure [9].
- A successful operative result depends on complete preoperative examination, correct staging of the deformity, and proper timing of treatment [10].
- One technique does not treat all deformities uniformly, highlighting the need to determine the true etiology before surgical intervention [12].
- Swan neck deformity can progress significantly with time due to increasing DIPJ flexion contracture [14].
Recovery¶
- Serial casting for adequate extension followed by 3 months of relative motion flexion (RMF) orthotic use yields similar results for chronic boutonniere deformity and should be attempted prior to surgical intervention [1].
- One to two grades of range of motion (ROM) improvement can be achieved with nonoperative treatment, although deformity can persist even after dedicated conservative management [8].
- The Y-shaped tendon graft is a useful procedure for the correction of chronic boutonniere deformity, providing good or excellent results in 16 of 18 patients in a reported series [6].
- The use of relative motion flexion orthoses (RMFO) is effective in increasing active distal interphalangeal joint flexion and improving proximal interphalangeal (PIP) extension in patients with Burton stage 1 chronic boutonniere deformity [13].
- Long-term results following soft tissue reconstruction for boutonniere deformity in rheumatoid arthritis are unreliable, and recurrent or persistent deformity is best treated with a salvage procedure [9].
- A successful operative result for boutonniere deformity depends on complete preoperative examination, correct staging of the deformity, and proper timing of treatment [10].
Key Evidence¶
- [L4] Similar results occurred for chronic boutonniere deformity using serial casting for adequate extension followed by 3 months of RMF orthotic use, which should be attempted prior to surgical intervention. (10.1016/j.jht.2023.02.005)
- [L5] Differentiating a true boutonniere deformity from a pseudoboutonniere injury is critical in determining clinical management. (10.1016/j.jhsa.2022.10.019)
- [L4] The natural history of the boutonnière deformity in rheumatoid arthritis is outlined, and a simple method of repair is described. (10.2106/00004623-196951070-00009)
- [L5] An understanding of the anatomy, clinical presentation, treatment options, and expected outcomes is crucial for optimal treatment of posttraumatic boutonnière and swan neck deformities. (10.5435/jaaos-d-14-00272)
- [L3] The prevalence of boutonnière deformity without rheumatoid arthritis or trauma is approximately 13%. (10.1177/1753193417704610)
- [L4] The Y-shaped tendon graft can be a useful procedure for the correction of chronic boutonniere deformity; in our patient series, this provided good or excellent results in 16 of 18 patients. (10.1016/j.jhsa.2021.01.003)
- [L5] Detachment of up to two-thirds of the phalangeal length was effective in reducing extensor lag of the DIP joint and did not cause any boutonniere deformity in this cadaveric model. (10.1016/j.jhsa.2012.07.039)
- [L3] One to two grades of ROM improvement can be achieved, although deformity can persist even after dedicated conservative management. (10.1016/j.jht.2025.02.013)
- [L5] Long-term results following soft tissue reconstruction are unreliable, and recurrent or persistent deformity is best treated with a salvage procedure. (10.1016/j.jhsa.2011.05.029)
- [L5] A successful operative result depends on complete preoperative examination, correct staging of the deformity, and proper timing of treatment. (10.5435/00124635-199903000-00002)
- [L5] Follow-up studies show that this surgery improves function and deformity and achieves nearly uniform patient satisfaction. (10.5435/00124635-200305000-00005)
- [L5] It emphasizes that one technique does not treat all deformities uniformly and highlights the need to determine the true etiology before surgical intervention. (10.1016/j.jhsa.2022.07.008)
- [L4] The use of RMFO is effective in increasing active distal interphalangeal joint flexion and improving PIP extension in patients with Burton stage 1 chronic boutonniere deformity. (10.1016/j.jhsa.2022.08.007)
- [L5] The swan neck deformity in this individual progressed significantly with time because of increasing DIPJ flexion contracture. (10.1016/j.jht.2009.11.005)
- [L5] Accurate diagnosis and treatment of finger metacarpophalangeal joint injuries in athletes begins with an understanding of all potential diagnoses, allowing for safe and early return to play. (10.5435/jaaos-d-21-01031)
- [L3] The modified classification could detect advanced deformity earlier and was more strongly correlated with hand function. (10.1177/1753193419886719)
- [L5] Hand surgery and hand therapy practice interventions, including use of RMF orthoses for management of non-surgical and surgical EM injuries may benefit from an in-depth look at the EM zone III and IV anatomy and biomechanics. (10.1016/j.jht.2023.01.002)
- [L4] The most important factor in the development of finger deformities is the changes occurring in the tendons and related structures, especially in early stages. (10.2106/00004623-195739030-00006)
- [L4] The modified technique provides a robust repair that anatomically mimics the extensor central slip yet maintains the function of the donor FDS tendon. (10.1016/j.jhsa.2009.01.025)
- [L5] The main goals of any treatment of a PIP joint complication are maintaining concentric reduction of the joint, restoring joint stability, and facilitating early range-of-motion exercises. (10.1016/j.hcl.2017.12.014)
- [L4] Cortical breaks were commonly visualized in MCP and PIP joints with HR-pQCT and microCT. (10.1186/s12891-016-1148-y)
References¶
[1] The relative motion concept in acute and chronic boutonniere deformity: Invited commentary. Journal of Hand Therapy. 2023. DOI: 10.1016/j.jht.2023.02.005 [2] Boutonniere Versus Pseudoboutonniere Deformities: Pathoanatomy, Diagnosis, and Treatment. The Journal of Hand Surgery. 2023. DOI: 10.1016/j.jhsa.2022.10.019 [3] Correction of the Rheumatoid Boutonnière Deformity. The Journal of Bone & Joint Surgery. 1969. DOI: 10.2106/00004623-196951070-00009 [4] Posttraumatic Boutonnière and Swan Neck Deformities. Journal of the American Academy of Orthopaedic Surgeons. 2015. DOI: 10.5435/jaaos-d-14-00272 [5] Thumb boutonnière deformity without rheumatoid arthritis or trauma. Journal of Hand Surgery (European Volume). 2017. DOI: 10.1177/1753193417704610 [6] Y-Shaped Tendon Graft—A Technique in the Reconstruction of Posttraumatic Chronic Boutonniere Deformity. The Journal of Hand Surgery. 2021. DOI: 10.1016/j.jhsa.2021.01.003 [7] Fractional Fowler Tenotomy for Chronic Mallet Finger: A Cadaveric Biomechanical Study. The Journal of Hand Surgery. 2012. DOI: 10.1016/j.jhsa.2012.07.039 [8] Nonoperative treatment of the Boutonniere deformity: Is there a difference in outcomes?. Journal of Hand Therapy. 2025. DOI: 10.1016/j.jht.2025.02.013 [9] Treatment of Boutonniere Finger Deformity in Rheumatoid Arthritis. The Journal of Hand Surgery. 2011. DOI: 10.1016/j.jhsa.2011.05.029 [10] Operative Correction of Swan-Neck and Boutonniere Deformities in the Rheumatoid Hand. Journal of the American Academy of Orthopaedic Surgeons. 1999. DOI: 10.5435/00124635-199903000-00002 [11] Metacarpophalangeal Joint Arthroplasty in Rheumatoid Arthritis. Journal of the American Academy of Orthopaedic Surgeons. 2003. DOI: 10.5435/00124635-200305000-00005 [12] Clarification of Extensor Tenotomy for Finger Deformities. The Journal of Hand Surgery. 2022. DOI: 10.1016/j.jhsa.2022.07.008 [13] The Use of Relative Motion Flexion Orthoses for Chronic Boutonniere Deformity. The Journal of Hand Surgery. 2024. DOI: 10.1016/j.jhsa.2022.08.007 [14] Swan Neck Deformity after Distal Interphalangeal Joint Flexion Contractures: A Biomechanical Analysis. Journal of Hand Therapy. 2010. DOI: 10.1016/j.jht.2009.11.005 [15] Finger Metacarpophalangeal Joint Injuries in Athletes: Evaluation, Diagnosis, Treatment, and Return to Play. Journal of the American Academy of Orthopaedic Surgeons. 2023. DOI: 10.5435/jaaos-d-21-01031 [17] A modified Terrono classification for Type 1 thumb deformity in rheumatoid arthritis: a cross-sectional analysis. Journal of Hand Surgery (European Volume). 2019. DOI: 10.1177/1753193419886719 [19] An in-depth look at zone III and IV anatomy of the finger extensor mechanism and some clinical implications for use of the relative motion flexion orthosis. Journal of Hand Therapy. 2023. DOI: 10.1016/j.jht.2023.01.002 [21] Finger Deformities Caused by Rheumatoid Arthritis. The Journal of Bone & Joint Surgery. 1957. DOI: 10.2106/00004623-195739030-00006 [24] Reconstruction of the Extensor Central Slip Using a Distally Based Flexor Digitorum Superficialis Slip. The Journal of Hand Surgery. 2009. DOI: 10.1016/j.jhsa.2009.01.025 [33] Complications of Proximal Interphalangeal Joint Injuries. Hand Clinics. 2018. DOI: 10.1016/j.hcl.2017.12.014 [37] Visual detection of cortical breaks in hand joints: reliability and validity of high-resolution peripheral quantitative CT compared to microCT. BMC Musculoskeletal Disorders. 2016. DOI: 10.1186/s12891-016-1148-y